
CT scan
| CT scan | |
|---|---|
 Modern CT scanner (2021), photon-counting CT (Siemens NAEOTOM Alpha) | |
| Other names | X-ray computed tomography (X-ray CT), computerized axial tomography scan (CAT scan),[1] computer aided tomography, computed tomography scan |
| ICD-10-PCS | B?2 |
| ICD-9-CM | 88.38 |
| MeSH | D014057 |
| OPS-301 code | 3–20...3–26 |
| MedlinePlus | 003330 |
A computed tomography scan (CT scan), formerly called computed axial tomography scan (CAT scan), is a medical imaging technique used to obtain detailed internal images of the body.[2] The personnel that perform CT scans are called radiographers or radiology technologists.[3][4]
CT scanners use a rotating X-ray tube and a row of detectors placed in a gantry to measure X-ray attenuations by different tissues inside the body. The multiple X-ray measurements taken from different angles are then processed on a computer using tomographic reconstruction algorithms to produce tomographic (cross-sectional) images (virtual "slices") of a body. CT scans can be used in patients with metallic implants or pacemakers, for whom magnetic resonance imaging (MRI) is contraindicated.
Since its development in the 1970s, CT scanning has proven to be a versatile imaging technique. While CT is most prominently used in medical diagnosis, it can also be used to form images of non-living objects. The 1979 Nobel Prize in Physiology or Medicine was awarded jointly to South African-American physicist Allan MacLeod Cormack and British electrical engineer Godfrey Hounsfield "for the development of computer-assisted tomography".[5][6]
Types
[edit]On the basis of image acquisition and procedures, various type of scanners are available in the market.
Sequential CT
[edit]Sequential CT, also known as step-and-shoot CT, is a type of scanning method in which the CT table moves stepwise. The table increments to a particular location and then stops which is followed by the X-ray tube rotation and acquisition of a slice. The table then increments again, and another slice is taken. The table movement stops while taking slices. This results in an increased time of scanning.[7]
Spiral CT
[edit]_and_patient_in_a_CT_imaging_system.gif)

Spinning tube, commonly called spiral CT, or helical CT, is an imaging technique in which an entire X-ray tube is spun around the central axis of the area being scanned. These are the dominant type of scanners on the market because they have been manufactured longer and offer a lower cost of production and purchase. The main limitation of this type of CT is the bulk and inertia of the equipment (X-ray tube assembly and detector array on the opposite side of the circle) which limits the speed at which the equipment can spin. Some designs use two X-ray sources and detector arrays offset by an angle, as a technique to improve temporal resolution.[8][9]
Electron beam tomography
[edit]Electron beam tomography (EBT) is a specific form of CT in which a large enough X-ray tube is constructed so that only the path of the electrons, travelling between the cathode and anode of the X-ray tube, are spun using deflection coils.[10] This type had a major advantage since sweep speeds can be much faster, allowing for less blurry imaging of moving structures, such as the heart and arteries.[11] Fewer scanners of this design have been produced when compared with spinning tube types, mainly due to the higher cost associated with building a much larger X-ray tube and detector array and limited anatomical coverage.[12]
Dual Energy CT
[edit]Dual Energy CT, also known as Spectral CT, is an advancement of Computed Tomography in which two energies are used to create two sets of data.[13] A Dual Energy CT may employ Dual source, Single source with dual detector layer, Single source with energy switching methods to get two different sets of data.[14]
- Dual source CT is an advanced scanner with a two X-ray tube detector system, unlike conventional single tube systems.[15][16] These two detector systems are mounted on a single gantry at 90° in the same plane.[17] Dual Source CT scanners allow fast scanning with higher temporal resolution by acquiring a full CT slice in only half a rotation. Fast imaging reduces motion blurring at high heart rates and potentially allowing for shorter breath-hold time. This is particularly useful for ill patients having difficulty holding their breath or unable to take heart-rate lowering medication.[17][18]
- Single Source with Energy switching is another mode of Dual energy CT in which a single tube is operated at two different energies by switching the energies frequently.[19][20]
CT perfusion imaging
[edit]
CT perfusion imaging is a specific form of CT to assess flow through blood vessels whilst injecting a contrast agent.[21] Blood flow, blood transit time, and organ blood volume, can all be calculated with reasonable sensitivity and specificity.[21] This type of CT may be used on the heart, although sensitivity and specificity for detecting abnormalities are still lower than for other forms of CT.[22] This may also be used on the brain, where CT perfusion imaging can often detect poor brain perfusion well before it is detected using a conventional spiral CT scan.[21][23] This is better for stroke diagnosis than other CT types.[23]
PET CT
[edit]
Positron emission tomography–computed tomography is a hybrid CT modality which combines, in a single gantry, a positron emission tomography (PET) scanner and an X-ray computed tomography (CT) scanner, to acquire sequential images from both devices in the same session, which are combined into a single superposed (co-registered) image. Thus, functional imaging obtained by PET, which depicts the spatial distribution of metabolic or biochemical activity in the body can be more precisely aligned or correlated with anatomic imaging obtained by CT scanning.[24]
PET-CT gives both anatomical and functional details of an organ under examination and is helpful in detecting different type of cancers.[25][26]
Medical use
[edit]Since its introduction in the 1970s,[27] CT has become an important tool in medical imaging to supplement conventional X-ray imaging and medical ultrasonography. It has more recently been used for preventive medicine or screening for disease, for example, CT colonography for people with a high risk of colon cancer, or full-motion heart scans for people with a high risk of heart disease. Several institutions offer full-body scans for the general population although this practice goes against the advice and official position of many professional organizations in the field primarily due to the radiation dose applied.[28]
The use of CT scans has increased dramatically over the last two decades in many countries.[29] An estimated 72 million scans were performed in the United States in 2007 and more than 80 million in 2015.[30][31]
Head
[edit]
CT scanning of the head is typically used to detect infarction (stroke), tumors, calcifications, haemorrhage, and bone trauma.[32] Of the above, hypodense (dark) structures can indicate edema and infarction, hyperdense (bright) structures indicate calcifications and haemorrhage and bone trauma can be seen as disjunction in bone windows. Tumors can be detected by the swelling and anatomical distortion they cause, or by surrounding edema. CT scanning of the head is also used in CT-guided stereotactic surgery and radiosurgery for treatment of intracranial tumors, arteriovenous malformations, and other surgically treatable conditions using a device known as the N-localizer.[33][34][35][36][37][38]
Neck
[edit]Contrast CT is generally the initial study of choice for neck masses in adults.[39] CT of the thyroid plays an important role in the evaluation of thyroid cancer.[40] CT scan often incidentally finds thyroid abnormalities, and so is often the preferred investigation modality for thyroid abnormalities.[40]
Lungs
[edit]A CT scan can be used for detecting both acute and chronic changes in the lung parenchyma, the tissue of the lungs.[41] It is particularly relevant here because normal two-dimensional X-rays do not show such defects. A variety of techniques are used, depending on the suspected abnormality. For evaluation of chronic interstitial processes such as emphysema, and fibrosis,[42] thin sections with high spatial frequency reconstructions are used; often scans are performed both on inspiration and expiration. This special technique is called high resolution CT that produces a sampling of the lung, and not continuous images.[43]

_and_diameter_(D).svg)
Bronchial wall thickening can be seen on lung CTs and generally (but not always) implies inflammation of the bronchi.[44]
An incidentally found nodule in the absence of symptoms (sometimes referred to as an incidentaloma) may raise concerns that it might represent a tumor, either benign or malignant.[45] Perhaps persuaded by fear, patients and doctors sometimes agree to an intensive schedule of CT scans, sometimes up to every three months and beyond the recommended guidelines, in an attempt to do surveillance on the nodules.[46] However, established guidelines advise that patients without a prior history of cancer and whose solid nodules have not grown over a two-year period are unlikely to have any malignant cancer.[46] For this reason, and because no research provides supporting evidence that intensive surveillance gives better outcomes, and because of risks associated with having CT scans, patients should not receive CT screening in excess of those recommended by established guidelines.[46]
Angiography
[edit]
Computed tomography angiography (CTA) is a type of contrast CT to visualize the arteries and veins throughout the body.[47] This ranges from arteries serving the brain to those bringing blood to the lungs, kidneys, arms and legs. An example of this type of exam is CT pulmonary angiogram (CTPA) used to diagnose pulmonary embolism (PE). It employs computed tomography and an iodine-based contrast agent to obtain an image of the pulmonary arteries.[48][49][50] CT scans can reduce the risk of angiography by providing clinicians with more information about the positioning and number of clots prior to the procedure.[51][52]
Cardiac
[edit]A CT scan of the heart is performed to gain knowledge about cardiac or coronary anatomy.[53] Traditionally, cardiac CT scans are used to detect, diagnose, or follow up coronary artery disease.[54] More recently CT has played a key role in the fast-evolving field of transcatheter structural heart interventions, more specifically in the transcatheter repair and replacement of heart valves.[55][56][57]
The main forms of cardiac CT scanning are:
- Coronary CT angiography (CCTA): the use of CT to assess the coronary arteries of the heart. The subject receives an intravenous injection of radiocontrast, and then the heart is scanned using a high-speed CT scanner, allowing radiologists to assess the extent of occlusion in the coronary arteries, usually to diagnose coronary artery disease.[58][59]
- Coronary CT calcium scan: also used for the assessment of severity of coronary artery disease. Specifically, it looks for calcium deposits in the coronary arteries that can narrow arteries and increase the risk of a heart attack.[60] A typical coronary CT calcium scan is done without the use of radiocontrast, but it can possibly be done from contrast-enhanced images as well.[61]
To better visualize the anatomy, post-processing of the images is common.[54] Most common are multiplanar reconstructions (MPR) and volume rendering. For more complex anatomies and procedures, such as heart valve interventions, a true 3D reconstruction or a 3D print is created based on these CT images to gain a deeper understanding.[62][63][64][65]
Abdomen and pelvis
[edit]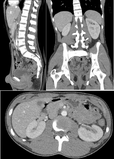
CT is an accurate technique for diagnosis of abdominal diseases like Crohn's disease,[66] GIT bleeding, and diagnosis and staging of cancer, as well as follow-up after cancer treatment to assess response.[67] It is commonly used to investigate acute abdominal pain.[68]
Non-enhanced computed tomography is today the gold standard for diagnosing urinary stones.[69] The size, volume and density of stones can be estimated to help clinicians guide further treatment; size is especially important in predicting spontaneous passage of a stone.[70]
Axial skeleton and extremities
[edit]For the axial skeleton and extremities, CT is often used to image complex fractures, especially ones around joints, because of its ability to reconstruct the area of interest in multiple planes. Fractures, ligamentous injuries, and dislocations can easily be recognized with a 0.2 mm resolution.[71][72] With modern dual-energy CT scanners, new areas of use have been established, such as aiding in the diagnosis of gout.[73]
Biomechanical use
[edit]CT is used in biomechanics to quickly reveal the geometry, anatomy, density and elastic moduli of biological tissues.[74][75]
Other uses
[edit]Industrial use
[edit]Industrial CT scanning (industrial computed tomography) is a process which uses X-ray equipment to produce 3D representations of components both externally and internally. Industrial CT scanning has been used in many areas of industry for internal inspection of components. Some of the key uses for CT scanning have been flaw detection, failure analysis, metrology, assembly analysis, image-based finite element methods[76] and reverse engineering applications. CT scanning is also employed in the imaging and conservation of museum artifacts.[77]
Aviation security
[edit]CT scanning has also found an application in transport security (predominantly airport security) where it is currently used in a materials analysis context for explosives detection CTX (explosive-detection device)[78][79][80][81] and is also under consideration for automated baggage/parcel security scanning using computer vision based object recognition algorithms that target the detection of specific threat items based on 3D appearance (e.g. guns, knives, liquid containers).[82][83][84] Its usage in airport security pioneered at Shannon Airport in March 2022 has ended the ban on liquids over 100 ml there, a move that Heathrow Airport plans for a full roll-out on 1 December 2022 and the TSA spent $781.2 million on an order for over 1,000 scanners, ready to go live in the summer.
Geological use
[edit]X-ray CT is used in geological studies to quickly reveal materials inside a drill core.[85] Dense minerals such as pyrite and barite appear brighter and less dense components such as clay appear dull in CT images.[86]
Paleontological use
[edit]Traditional methods of studying fossils are often destructive, such as the use of thin sections and physical preparation. X-ray CT is used in paleontology to non-destructively visualize fossils in 3D.[87] This has many advantages. For example, we can look at fragile structures that might never otherwise be able to be studied. In addition, one can freely move around models of fossils in virtual 3D space to inspect it without damaging the fossil.
Cultural heritage use
[edit]X-ray CT and micro-CT can also be used for the conservation and preservation of objects of cultural heritage. For many fragile objects, direct research and observation can be damaging and can degrade the object over time. Using CT scans, conservators and researchers are able to determine the material composition of the objects they are exploring, such as the position of ink along the layers of a scroll, without any additional harm. These scans have been optimal for research focused on the workings of the Antikythera mechanism or the text hidden inside the charred outer layers of the En-Gedi Scroll. However, they are not optimal for every object subject to these kinds of research questions, as there are certain artifacts like the Herculaneum papyri in which the material composition has very little variation along the inside of the object. After scanning these objects, computational methods can be employed to examine the insides of these objects, as was the case with the virtual unwrapping of the En-Gedi scroll and the Herculaneum papyri.[88] Micro-CT has also proved useful for analyzing more recent artifacts such as still-sealed historic correspondence that employed the technique of letterlocking (complex folding and cuts) that provided a "tamper-evident locking mechanism".[89][90] Further examples of use cases in archaeology is imaging the contents of sarcophagi or ceramics.[91]
Recently, CWI in Amsterdam has collaborated with Rijksmuseum to investigate art object inside details in the framework called IntACT.[92]
Micro organism research
[edit]Varied types of fungus can degrade wood to different degrees, one Belgium research group has been used X-ray CT 3 dimension with sub-micron resolution unveiled fungi can penetrate micropores of 0.6 μm[93] under certain conditions.
Timber sawmill
[edit]Sawmills use industrial CT scanners to detect round defects, for instance knots, to improve total value of timber productions. Most sawmills are planning to incorporate this robust detection tool to improve productivity in the long run, however initial investment cost is high.[citation needed]
Interpretation of results
[edit]Presentation
[edit]
− Average intensity projection
− Maximum intensity projection
− Thin slice (median plane)
− Volume rendering by high and low threshold for radiodensity
The result of a CT scan is a volume of voxels, which may be presented to a human observer by various methods, which broadly fit into the following categories:
- Slices (of varying thickness). Thin slice is generally regarded as planes representing a thickness of less than 3 mm.[94][95] Thick slice is generally regarded as planes representing a thickness between 3 mm and 5 mm.[95][96]
- Projection, including maximum intensity projection[97] and average intensity projection
- Volume rendering (VR)[97]
Technically, all volume renderings become projections when viewed on a 2-dimensional display, making the distinction between projections and volume renderings a bit vague. The epitomes of volume rendering models feature a mix of for example coloring and shading in order to create realistic and observable representations.[98][99]
Two-dimensional CT images are conventionally rendered so that the view is as though looking up at it from the patient's feet.[100] Hence, the left side of the image is to the patient's right and vice versa, while anterior in the image also is the patient's anterior and vice versa. This left-right interchange corresponds to the view that physicians generally have in reality when positioned in front of patients.[101]
Grayscale
[edit]Pixels in an image obtained by CT scanning are displayed in terms of relative radiodensity. The pixel itself is displayed according to the mean attenuation of the tissue(s) that it corresponds to on a scale from +3,071 (most attenuating) to −1,024 (least attenuating) on the Hounsfield scale. A pixel is a two dimensional unit based on the matrix size and the field of view. When the CT slice thickness is also factored in, the unit is known as a voxel, which is a three-dimensional unit.[102] Water has an attenuation of 0 Hounsfield units (HU), while air is −1,000 HU, cancellous bone is typically +400 HU, and cranial bone can reach 2,000 HU.[103] The attenuation of metallic implants depends on the atomic number of the element used: Titanium usually has an amount of +1000 HU, iron steel can completely block the X-ray and is, therefore, responsible for well-known line-artifacts in computed tomograms. Artifacts are caused by abrupt transitions between low- and high-density materials, which results in data values that exceed the dynamic range of the processing electronics.[104]
Windowing
[edit]CT data sets have a very high dynamic range which must be reduced for display or printing. This is typically done via a process of "windowing", which maps a range (the "window") of pixel values to a grayscale ramp. For example, CT images of the brain are commonly viewed with a window extending from 0 HU to 80 HU. Pixel values of 0 and lower, are displayed as black; values of 80 and higher are displayed as white; values within the window are displayed as a gray intensity proportional to position within the window.[105] The window used for display must be matched to the X-ray density of the object of interest, in order to optimize the visible detail.[106] Window width and window level parameters are used to control the windowing of a scan.[107]
Multiplanar reconstruction and projections
[edit]

Multiplanar reconstruction (MPR) is the process of converting data from one anatomical plane (usually transverse) to other planes. It can be used for thin slices as well as projections. Multiplanar reconstruction is possible as present CT scanners provide almost isotropic resolution.[108]
MPR is used almost in every scan. The spine is frequently examined with it.[109] An image of the spine in axial plane can only show one vertebral bone at a time and cannot show its relation with other vertebral bones. By reformatting the data in other planes, visualization of the relative position can be achieved in sagittal and coronal plane.[110]
New software allows the reconstruction of data in non-orthogonal (oblique) planes, which help in the visualization of organs which are not in orthogonal planes.[111][112] It is better suited for visualization of the anatomical structure of the bronchi as they do not lie orthogonal to the direction of the scan.[113]
Curved-plane reconstruction (or curved planar reformation = CPR) is performed mainly for the evaluation of vessels. This type of reconstruction helps to straighten the bends in a vessel, thereby helping to visualize a whole vessel in a single image or in multiple images. After a vessel has been "straightened", measurements such as cross-sectional area and length can be made. This is helpful in preoperative assessment of a surgical procedure.[114]
For 2D projections used in radiation therapy for quality assurance and planning of external beam radiotherapy, including digitally reconstructed radiographs, see Beam's eye view.
| Type of projection | Schematic illustration | Examples (10 mm slabs) | Description | Uses |
|---|---|---|---|---|
| Average intensity projection (AIP) | 
|
The average attenuation of each voxel is displayed. The image will get smoother as slice thickness increases. It will look more and more similar to conventional projectional radiography as slice thickness increases. | Useful for identifying the internal structures of a solid organ or the walls of hollow structures, such as intestines. | |
| Maximum intensity projection (MIP) | 
|
The voxel with the highest attenuation is displayed. Therefore, high-attenuating structures such as blood vessels filled with contrast media are enhanced. | Useful for angiographic studies and identification of pulmonary nodules. | |
| Minimum intensity projection (MinIP) | 
|
The voxel with the lowest attenuation is displayed. Therefore, low-attenuating structures such as air spaces are enhanced. | Useful for assessing the lung parenchyma. |
Volume rendering
[edit]
A threshold value of radiodensity is set by the operator (e.g., a level that corresponds to bone). With the help of edge detection image processing algorithms a 3D model can be constructed from the initial data and displayed on screen. Various thresholds can be used to get multiple models, each anatomical component such as muscle, bone and cartilage can be differentiated on the basis of different colours given to them. However, this mode of operation cannot show interior structures.[116]
Surface rendering is limited technique as it displays only the surfaces that meet a particular threshold density, and which are towards the viewer. However, In volume rendering, transparency, colours and shading are used which makes it easy to present a volume in a single image. For example, Pelvic bones could be displayed as semi-transparent, so that, even viewing at an oblique angle one part of the image does not hide another.[117]
Image quality
[edit]Dose versus image quality
[edit]An important issue within radiology today is how to reduce the radiation dose during CT examinations without compromising the image quality. In general, higher radiation doses result in higher-resolution images,[118] while lower doses lead to increased image noise and unsharp images. However, increased dosage raises the adverse side effects, including the risk of radiation-induced cancer – a four-phase abdominal CT gives the same radiation dose as 300 chest X-rays.[119] Several methods that can reduce the exposure to ionizing radiation during a CT scan exist.[120]
- New software technology can significantly reduce the required radiation dose. New iterative tomographic reconstruction algorithms (e.g., iterative Sparse Asymptotic Minimum Variance) could offer super-resolution without requiring higher radiation dose.[121]
- Individualize the examination and adjust the radiation dose to the body type and body organ examined. Different body types and organs require different amounts of radiation.[122]
- Higher resolution is not always suitable, such as detection of small pulmonary masses.[123]
Artifacts
[edit]Although images produced by CT are generally faithful representations of the scanned volume, the technique is susceptible to a number of artifacts, such as the following:[124][125]Chapters 3 and 5
- Streak artifact
- Streaks are often seen around materials that block most X-rays, such as metal or bone. Numerous factors contribute to these streaks: under sampling, photon starvation, motion, beam hardening, and Compton scatter. This type of artifact commonly occurs in the posterior fossa of the brain, or if there are metal implants. The streaks can be reduced using newer reconstruction techniques.[126] Approaches such as metal artifact reduction (MAR) can also reduce this artifact.[127][128] MAR techniques include spectral imaging, where CT images are taken with photons of different energy levels, and then synthesized into monochromatic images with special software such as GSI (Gemstone Spectral Imaging).[129]
- Partial volume effect
- This appears as "blurring" of edges. It is due to the scanner being unable to differentiate between a small amount of high-density material (e.g., bone) and a larger amount of lower density (e.g., cartilage).[130] The reconstruction assumes that the X-ray attenuation within each voxel is homogeneous; this may not be the case at sharp edges. This is most commonly seen in the z-direction (craniocaudal direction), due to the conventional use of highly anisotropic voxels, which have a much lower out-of-plane resolution, than in-plane resolution. This can be partially overcome by scanning using thinner slices, or an isotropic acquisition on a modern scanner.[131]
- Ring artifact
- Probably the most common mechanical artifact, the image of one or many "rings" appears within an image. They are usually caused by the variations in the response from individual elements in a two dimensional X-ray detector due to defect or miscalibration.[132] Ring artifacts can largely be reduced by intensity normalization, also referred to as flat field correction.[133] Remaining rings can be suppressed by a transformation to polar space, where they become linear stripes.[132] A comparative evaluation of ring artefact reduction on X-ray tomography images showed that the method of Sijbers and Postnov can effectively suppress ring artefacts.[134]
- Noise
- This appears as grain on the image and is caused by a low signal to noise ratio. This occurs more commonly when a thin slice thickness is used. It can also occur when the power supplied to the X-ray tube is insufficient to penetrate the anatomy.[135]
- Windmill
- Streaking appearances can occur when the detectors intersect the reconstruction plane. This can be reduced with filters or a reduction in pitch.[136][137]
- Beam hardening
- This can give a "cupped appearance" when grayscale is visualized as height. It occurs because conventional sources, like X-ray tubes emit a polychromatic spectrum. Photons of higher photon energy levels are typically attenuated less. Because of this, the mean energy of the spectrum increases when passing the object, often described as getting "harder". This leads to an effect increasingly underestimating material thickness, if not corrected. Many algorithms exist to correct for this artifact. They can be divided into mono- and multi-material methods.[126][138][139]
Advantages
[edit]CT scanning has several advantages over traditional two-dimensional medical radiography. First, CT eliminates the superimposition of images of structures outside the area of interest.[140] Second, CT scans have greater image resolution, enabling examination of finer details. CT can distinguish between tissues that differ in radiographic density by 1% or less.[141] Third, CT scanning enables multiplanar reformatted imaging: scan data can be visualized in the transverse (or axial), coronal, or sagittal plane, depending on the diagnostic task.[142]
The improved resolution of CT has permitted the development of new investigations. For example, CT angiography avoids the invasive insertion of a catheter. CT scanning can perform a virtual colonoscopy with greater accuracy and less discomfort for the patient than a traditional colonoscopy.[143][144] Virtual colonography is far more accurate than a barium enema for detection of tumors and uses a lower radiation dose.[145]
CT is a moderate-to-high radiation diagnostic technique. The radiation dose for a particular examination depends on multiple factors: volume scanned, patient build, number and type of scan protocol, and desired resolution and image quality.[146] Two helical CT scanning parameters, tube current and pitch, can be adjusted easily and have a profound effect on radiation. CT scanning is more accurate than two-dimensional radiographs in evaluating anterior interbody fusion, although they may still over-read the extent of fusion.[147]
Adverse effects
[edit]Cancer
[edit]The radiation used in CT scans can damage body cells, including DNA molecules, which can lead to radiation-induced cancer.[148] The radiation doses received from CT scans is variable. Compared to the lowest dose X-ray techniques, CT scans can have 100 to 1,000 times higher dose than conventional X-rays.[149] However, a lumbar spine X-ray has a similar dose as a head CT.[150] Articles in the media often exaggerate the relative dose of CT by comparing the lowest-dose X-ray techniques (chest X-ray) with the highest-dose CT techniques. In general, a routine abdominal CT has a radiation dose similar to three years of average background radiation.[151]
Large scale population-based studies have consistently demonstrated that low dose radiation from CT scans has impacts on cancer incidence in a variety of cancers.[152][153][154][155] For example, in a large population-based Australian cohort it was found that up to 3.7% of brain cancers were caused by CT scan radiation.[156] Some experts project that in the future, between three and five percent of all cancers would result from medical imaging.[149] An Australian study of 10.9 million people reported that the increased incidence of cancer after CT scan exposure in this cohort was mostly due to irradiation. In this group, one in every 1,800 CT scans was followed by an excess cancer. If the lifetime risk of developing cancer is 40% then the absolute risk rises to 40.05% after a CT. The risks of CT scan radiation are especially important in patients undergoing recurrent CT scans within a short time span of one to five years.[157][158][159]
Some experts note that CT scans are known to be "overused," and "there is distressingly little evidence of better health outcomes associated with the current high rate of scans."[149] On the other hand, a recent paper analyzing the data of patients who received high cumulative doses showed a high degree of appropriate use.[160] This creates an important issue of cancer risk to these patients. Moreover, a highly significant finding that was previously unreported is that some patients received >100 mSv dose from CT scans in a single day,[158] which counteracts existing criticisms some investigators may have on the effects of protracted versus acute exposure.
There are contrarian views and the debate is ongoing. Some studies have shown that publications indicating an increased risk of cancer from typical doses of body CT scans are plagued with serious methodological limitations and several highly improbable results,[161] concluding that no evidence indicates such low doses cause any long-term harm.[162][163][164] One study estimated that as many as 0.4% of cancers in the United States resulted from CT scans, and that this may have increased to as much as 1.5 to 2% based on the rate of CT use in 2007.[148] Others dispute this estimate,[165] as there is no consensus that the low levels of radiation used in CT scans cause damage. Lower radiation doses are used in many cases, such as in the investigation of renal colic.[166]
A person's age plays a significant role in the subsequent risk of cancer.[167] Estimated lifetime cancer mortality risks from an abdominal CT of a one-year-old is 0.1%, or 1:1000 scans.[167] The risk for someone who is 40 years old is half that of someone who is 20 years old with substantially less risk in the elderly.[167] The International Commission on Radiological Protection estimates that the risk to a fetus being exposed to 10 mGy (a unit of radiation exposure) increases the rate of cancer before 20 years of age from 0.03% to 0.04% (for reference a CT pulmonary angiogram exposes a fetus to 4 mGy).[168] A 2012 review did not find an association between medical radiation and cancer risk in children noting however the existence of limitations in the evidences over which the review is based.[169] CT scans can be performed with different settings for lower exposure in children with most manufacturers of CT scans as of 2007 having this function built in.[170] Furthermore, certain conditions can require children to be exposed to multiple CT scans.[148]
Current recommendations are to inform patients of the risks of CT scanning.[171] However, employees of imaging centers tend not to communicate such risks unless patients ask.[172]
Contrast reactions
[edit]In the United States half of CT scans are contrast CTs using intravenously injected radiocontrast agents.[173] The most common reactions from these agents are mild, including nausea, vomiting, and an itching rash. Severe life-threatening reactions may rarely occur.[174] Overall reactions occur in 1 to 3% with nonionic contrast and 4 to 12% of people with ionic contrast.[175] Skin rashes may appear within a week to 3% of people.[174]
The old radiocontrast agents caused anaphylaxis in 1% of cases while the newer, low-osmolar agents cause reactions in 0.01–0.04% of cases.[174][176] Death occurs in about 2 to 30 people per 1,000,000 administrations, with newer agents being safer.[175][177] There is a higher risk of mortality in those who are female, elderly or in poor health, usually secondary to either anaphylaxis or acute kidney injury.[173]
The contrast agent may induce contrast-induced nephropathy.[178] This occurs in 2 to 7% of people who receive these agents, with greater risk in those who have preexisting kidney failure,[178] preexisting diabetes, or reduced intravascular volume. People with mild kidney impairment are usually advised to ensure full hydration for several hours before and after the injection. For moderate kidney failure, the use of iodinated contrast should be avoided; this may mean using an alternative technique instead of CT. Those with severe kidney failure requiring dialysis require less strict precautions, as their kidneys have so little function remaining that any further damage would not be noticeable and the dialysis will remove the contrast agent; it is normally recommended, however, to arrange dialysis as soon as possible following contrast administration to minimize any adverse effects of the contrast.
In addition to the use of intravenous contrast, orally administered contrast agents are frequently used when examining the abdomen.[179] These are frequently the same as the intravenous contrast agents, merely diluted to approximately 10% of the concentration. However, oral alternatives to iodinated contrast exist, such as very dilute (0.5–1% w/v) barium sulfate suspensions. Dilute barium sulfate has the advantage that it does not cause allergic-type reactions or kidney failure, but cannot be used in patients with suspected bowel perforation or suspected bowel injury, as leakage of barium sulfate from damaged bowel can cause fatal peritonitis.[180]
Side effects from contrast agents, administered intravenously in some CT scans, might impair kidney performance in patients with kidney disease, although this risk is now believed to be lower than previously thought.[181][178]
Scan dose
[edit]| Examination | Typical effective dose (mSv) to the whole body |
Typical absorbed dose (mGy) to the organ in question |
|---|---|---|
| Annual background radiation | 2.4[182] | 2.4[182] |
| Chest X-ray | 0.02[183] | 0.01–0.15[184] |
| Head CT | 1–2[167] | 56[185] |
| Screening mammography | 0.4[168] | 3[148][184] |
| Abdominal CT | 8[183] | 14[185] |
| Chest CT | 5–7[167] | 13[185] |
| CT colonography | 6–11[167] | |
| Chest, abdomen and pelvis CT | 9.9[185] | 12[185] |
| Cardiac CT angiogram | 9–12[167] | 40–100[184] |
| Barium enema | 15[148] | 15[184] |
| Neonatal abdominal CT | 20[148] | 20[184] |
The table reports average radiation exposures; however, there can be a wide variation in radiation doses between similar scan types, where the highest dose could be as much as 22 times higher than the lowest dose.[167] A typical plain film X-ray involves radiation dose of 0.01 to 0.15 mGy, while a typical CT can involve 10–20 mGy for specific organs, and can go up to 80 mGy for certain specialized CT scans.[184]
For purposes of comparison, the world average dose rate from naturally occurring sources of background radiation is 2.4 mSv per year, equal for practical purposes in this application to 2.4 mGy per year.[182] While there is some variation, most people (99%) received less than 7 mSv per year as background radiation.[186] Medical imaging as of 2007 accounted for half of the radiation exposure of those in the United States with CT scans making up two thirds of this amount.[167] In the United Kingdom it accounts for 15% of radiation exposure.[168] The average radiation dose from medical sources is ≈0.6 mSv per person globally as of 2007.[167] Those in the nuclear industry in the United States are limited to doses of 50 mSv a year and 100 mSv every 5 years.[167]
Lead is the main material used by radiography personnel for shielding against scattered X-rays.
Radiation dose units
[edit]The radiation dose reported in the gray or mGy unit is proportional to the amount of energy that the irradiated body part is expected to absorb, and the physical effect (such as DNA double strand breaks) on the cells' chemical bonds by X-ray radiation is proportional to that energy.[187]
The sievert unit is used in the report of the effective dose. The sievert unit, in the context of CT scans, does not correspond to the actual radiation dose that the scanned body part absorbs but to another radiation dose of another scenario, the whole body absorbing the other radiation dose and the other radiation dose being of a magnitude, estimated to have the same probability to induce cancer as the CT scan.[188] Thus, as is shown in the table above, the actual radiation that is absorbed by a scanned body part is often much larger than the effective dose suggests. A specific measure, termed the computed tomography dose index (CTDI), is commonly used as an estimate of the radiation absorbed dose for tissue within the scan region, and is automatically computed by medical CT scanners.[189]
The equivalent dose is the effective dose of a case, in which the whole body would actually absorb the same radiation dose, and the sievert unit is used in its report. In the case of non-uniform radiation, or radiation given to only part of the body, which is common for CT examinations, using the local equivalent dose alone would overstate the biological risks to the entire organism.[190][191][192]
Effects of radiation
[edit]Most adverse health effects of radiation exposure may be grouped in two general categories:
- deterministic effects (harmful tissue reactions) due in large part to the killing/malfunction of cells following high doses;[193]
- stochastic effects, i.e., cancer and heritable effects involving either cancer development in exposed individuals owing to mutation of somatic cells or heritable disease in their offspring owing to mutation of reproductive (germ) cells.[194]
The added lifetime risk of developing cancer by a single abdominal CT of 8 mSv is estimated to be 0.05%, or 1 one in 2,000.[195]
Because of increased susceptibility of fetuses to radiation exposure, the radiation dosage of a CT scan is an important consideration in the choice of medical imaging in pregnancy.[196][197]
Excess doses
[edit]In October, 2009, the US Food and Drug Administration (FDA) initiated an investigation of brain perfusion CT (PCT) scans, based on radiation burns caused by incorrect settings at one particular facility for this particular type of CT scan. Over 200 patients were exposed to radiation at approximately eight times the expected dose for an 18-month period; over 40% of them lost patches of hair. This event prompted a call for increased CT quality assurance programs. It was noted that "while unnecessary radiation exposure should be avoided, a medically needed CT scan obtained with appropriate acquisition parameter has benefits that outweigh the radiation risks."[167][198] Similar problems have been reported at other centers.[167] These incidents are believed to be due to human error.[167]
Procedure
[edit]CT scan procedure varies according to the type of the study and the organ being imaged. The patient is made to lie on the CT table and the centering of the table is done according to the body part. The IV line is established in case of contrast-enhanced CT. After selecting proper[clarification needed] and rate of contrast from the pressure injector, the scout is taken to localize and plan the scan. Once the plan is selected, the contrast is given. The raw data is processed according to the study and proper windowing is done to make scans easy to diagnose.[199]
Preparation
[edit]Patient preparation may vary according to the type of scan. The general patient preparation includes.[199]
- Signing the informed consent.
- Removal of metallic objects and jewelry from the region of interest.
- Changing to the hospital gown according to hospital protocol.
- Checking of kidney function, especially creatinine and urea levels (in case of CECT).[200]
Mechanism
[edit]
T: X-ray tube
D: X-ray detectors
X: X-ray beam
R: Gantry rotation

Computed tomography operates by using an X-ray generator that rotates around the object; X-ray detectors are positioned on the opposite side of the circle from the X-ray source.[202] As the X-rays pass through the patient, they are attenuated differently by various tissues according to the tissue density.[203] A visual representation of the raw data obtained is called a sinogram, yet it is not sufficient for interpretation.[204] Once the scan data has been acquired, the data must be processed using a form of tomographic reconstruction, which produces a series of cross-sectional images.[205] These cross-sectional images are made up of small units of pixels or voxels.[206]
Pixels in an image obtained by CT scanning are displayed in terms of relative radiodensity. The pixel itself is displayed according to the mean attenuation of the tissue(s) that it corresponds to on a scale from +3,071 (most attenuating) to −1,024 (least attenuating) on the Hounsfield scale. A pixel is a two dimensional unit based on the matrix size and the field of view. When the CT slice thickness is also factored in, the unit is known as a voxel, which is a three-dimensional unit.[206]
Water has an attenuation of 0 Hounsfield units (HU), while air is −1,000 HU, cancellous bone is typically +400 HU, and cranial bone can reach 2,000 HU or more (os temporale) and can cause artifacts. The attenuation of metallic implants depends on the atomic number of the element used: Titanium usually has an amount of +1000 HU, iron steel can completely extinguish the X-ray and is, therefore, responsible for well-known line-artifacts in computed tomograms. Artifacts are caused by abrupt transitions between low- and high-density materials, which results in data values that exceed the dynamic range of the processing electronics. Two-dimensional CT images are conventionally rendered so that the view is as though looking up at it from the patient's feet.[100] Hence, the left side of the image is to the patient's right and vice versa, while anterior in the image also is the patient's anterior and vice versa. This left-right interchange corresponds to the view that physicians generally have in reality when positioned in front of patients.
Initially, the images generated in CT scans were in the transverse (axial) anatomical plane, perpendicular to the long axis of the body. Modern scanners allow the scan data to be reformatted as images in other planes. Digital geometry processing can generate a three-dimensional image of an object inside the body from a series of two-dimensional radiographic images taken by rotation around a fixed axis.[124] These cross-sectional images are widely used for medical diagnosis and therapy.[207]
Contrast
[edit]Contrast media used for X-ray CT, as well as for plain film X-ray, are called radiocontrasts. Radiocontrasts for CT are, in general, iodine-based.[208] This is useful to highlight structures such as blood vessels that otherwise would be difficult to delineate from their surroundings. Using contrast material can also help to obtain functional information about tissues. Often, images are taken both with and without radiocontrast.[209]
History
[edit]The history of X-ray computed tomography goes back to at least 1917 with the mathematical theory of the Radon transform.[210][211] In October 1963, William H. Oldendorf received a U.S. patent for a "radiant energy apparatus for investigating selected areas of interior objects obscured by dense material".[212] The first commercially viable CT scanner was invented by Godfrey Hounsfield in 1972.[213]
It is often claimed that revenues from the sales of The Beatles' records in the 1960s helped fund the development of the first CT scanner at EMI. The first production X-ray CT machines were in fact called EMI scanners.[214]
Etymology
[edit]The word tomography is derived from the Greek tome 'slice' and graphein 'to write'.[215] Computed tomography was originally known as the "EMI scan" as it was developed in the early 1970s at a research branch of EMI, a company best known today for its music and recording business.[216] It was later known as computed axial tomography (CAT or CT scan) and body section röntgenography.[217]
The term CAT scan is no longer in technical use because current CT scans enable for multiplanar reconstructions. This makes CT scan the most appropriate term, which is used by radiologists in common vernacular as well as in textbooks and scientific papers.[218][219][220]
In Medical Subject Headings (MeSH), computed axial tomography was used from 1977 to 1979, but the current indexing explicitly includes X-ray in the title.[221]
The term sinogram was introduced by Paul Edholm and Bertil Jacobson in 1975.[222]
Society and culture
[edit]| Country | Value |
|---|---|
| 111.49 | |
| 64.35 | |
| 43.68 | |
| 42.64 | |
| 39.72 | |
| 39.28 | |
| 39.13 | |
| 38.18 | |
| 35.13 | |
| 34.71 | |
| 34.22 | |
| 28.64 | |
| 24.51 | |
| 24.27 | |
| 23.33 | |
| 19.14 | |
| 18.59 | |
| 18.22 | |
| 17.36 | |
| 17.28 | |
| 16.88 | |
| 16.77 | |
| 16.69 | |
| 15.76 | |
| 15.28 | |
| 15.00 | |
| 14.77 | |
| 13.48 | |
| 13.00 | |
| 9.53 | |
| 9.19 | |
| 5.83 | |
| 1.24 |
Campaigns
[edit]In response to increased concern by the public and the ongoing progress of best practices, the Alliance for Radiation Safety in Pediatric Imaging was formed within the Society for Pediatric Radiology. In concert with the American Society of Radiologic Technologists, the American College of Radiology and the American Association of Physicists in Medicine, the Society for Pediatric Radiology developed and launched the Image Gently Campaign which is designed to maintain high-quality imaging studies while using the lowest doses and best radiation safety practices available on pediatric patients.[224] This initiative has been endorsed and applied by a growing list of various professional medical organizations around the world and has received support and assistance from companies that manufacture equipment used in Radiology.
Following upon the success of the Image Gently campaign, the American College of Radiology, the Radiological Society of North America, the American Association of Physicists in Medicine and the American Society of Radiologic Technologists have launched a similar campaign to address this issue in the adult population called Image Wisely.[225]
The World Health Organization and International Atomic Energy Agency (IAEA) of the United Nations have also been working in this area and have ongoing projects designed to broaden best practices and lower patient radiation dose.[226][227]
Prevalence
[edit]Use of CT has increased dramatically over the last two decades.[29] An estimated 72 million scans were performed in the United States in 2007,[30] accounting for close to half of the total per-capita dose rate from radiologic and nuclear medicine procedures.[228] Of the CT scans, six to eleven percent are done in children,[168] an increase of seven to eightfold from 1980.[167] Similar increases have been seen in Europe and Asia.[167] In Calgary, Canada, 12.1% of people who present to the emergency with an urgent complaint received a CT scan, most commonly either of the head or of the abdomen. The percentage who received CT, however, varied markedly by the emergency physician who saw them from 1.8% to 25%.[229] In the emergency department in the United States, CT or MRI imaging is done in 15% of people who present with injuries as of 2007 (up from 6% in 1998).[230]
The increased use of CT scans has been the greatest in two fields: screening of adults (screening CT of the lung in smokers, virtual colonoscopy, CT cardiac screening, and whole-body CT in asymptomatic patients) and CT imaging of children. Shortening of the scanning time to around 1 second, eliminating the strict need for the subject to remain still or be sedated, is one of the main reasons for the large increase in the pediatric population (especially for the diagnosis of appendicitis).[148] As of 2007, in the United States a proportion of CT scans are performed unnecessarily.[170] Some estimates place this number at 30%.[168] There are a number of reasons for this including: legal concerns, financial incentives, and desire by the public.[170] For example, some healthy people avidly pay to receive full-body CT scans as screening. In that case, it is not at all clear that the benefits outweigh the risks and costs. Deciding whether and how to treat incidentalomas is complex, radiation exposure is not negligible, and the money for the scans involves opportunity cost.[170]
Manufacturers
[edit]Major manufacturers of CT scanning devices and equipment are:[231]
 GE HealthCare
GE HealthCare Siemens Healthineers
Siemens Healthineers Canon Medical Systems Corporation (formerly Toshiba Medical Systems)
Canon Medical Systems Corporation (formerly Toshiba Medical Systems) Koninklijke Philips N.V.
Koninklijke Philips N.V.- Fujifilm Healthcare (formerly Hitachi Medical Systems)
 Neusoft Medical Systems
Neusoft Medical Systems- United Imaging
Research
[edit]Photon-counting computed tomography is a CT technique currently under development.[as of?] Typical CT scanners use energy integrating detectors; photons are measured as a voltage on a capacitor which is proportional to the X-rays detected. However, this technique is susceptible to noise and other factors which can affect the linearity of the voltage to X-ray intensity relationship.[232] Photon counting detectors (PCDs) are still affected by noise but it does not change the measured counts of photons. PCDs have several potential advantages, including improving signal (and contrast) to noise ratios, reducing doses, improving spatial resolution, and through use of several energies, distinguishing multiple contrast agents.[233][234] PCDs have only recently become feasible in CT scanners due to improvements in detector technologies that can cope with the volume and rate of data required. As of February 2016, photon counting CT is in use at three sites.[235] Some early research has found the dose reduction potential of photon counting CT for breast imaging to be very promising.[236] In view of recent findings of high cumulative doses to patients from recurrent CT scans, there has been a push for scanning technologies and techniques that reduce ionising radiation doses to patients to sub-milliSievert (sub-mSv in the literature) levels during the CT scan process, a goal that has been lingering.[237][158][159][160]
See also
[edit]References
[edit]- ^ "CT scan – Mayo Clinic". mayoclinic.org. Archived from the original on 15 October 2016. Retrieved 20 October 2016.
- ^ Hermena S, Young M (2022), "CT-scan Image Production Procedures", StatPearls, Treasure Island, Florida: StatPearls Publishing, PMID 34662062, retrieved 2023-11-24
- ^ "Patient Page". ARRT – The American Registry of Radiologic Technologists. Archived from the original on 9 November 2014.
- ^ "Individual State Licensure Information". American Society of Radiologic Technologists. Archived from the original on 18 July 2013. Retrieved 19 July 2013.
- ^ "The Nobel Prize in Physiology or Medicine 1979". NobelPrize.org. Retrieved 2019-08-10.
- ^ "The Nobel Prize in Physiology or Medicine 1979". NobelPrize.org. Retrieved 2023-10-28.
- ^ Terrier F, Grossholz M, Becker CD (2012-12-06). Spiral CT of the Abdomen. Springer Science & Business Media. p. 4. ISBN 978-3-642-56976-0.
- ^ Fishman EK, Jeffrey RB (1995). Spiral CT: Principles, Techniques, and Clinical Applications. Raven Press. ISBN 978-0-7817-0218-8.
- ^ Hsieh J (2003). Computed Tomography: Principles, Design, Artifacts, and Recent Advances. SPIE Press. p. 265. ISBN 978-0-8194-4425-7.
- ^ Stirrup J (2020-01-02). Cardiovascular Computed Tomography. Oxford University Press. ISBN 978-0-19-880927-2.
- ^ Talisetti A, Jelnin V, Ruiz C, John E, Benedetti E, Testa G, Holterman AX, Holterman MJ (December 2004). "Electron beam CT scan is a valuable and safe imaging tool for the pediatric surgical patient". Journal of Pediatric Surgery. 39 (12): 1859–1862. doi:10.1016/j.jpedsurg.2004.08.024. ISSN 1531-5037. PMID 15616951.
- ^ Retsky M (31 July 2008). "Electron beam computed tomography: Challenges and opportunities". Physics Procedia. 1 (1): 149–154. Bibcode:2008PhPro...1..149R. doi:10.1016/j.phpro.2008.07.090.
- ^ Johnson T, Fink C, Schönberg SO, Reiser MF (2011-01-18). Dual Energy CT in Clinical Practice. Springer Science & Business Media. ISBN 978-3-642-01740-7.
- ^ Johnson T, Fink C, Schönberg SO, Reiser MF (2011-01-18). Dual Energy CT in Clinical Practice. Springer Science & Business Media. p. 8. ISBN 978-3-642-01740-7.
- ^ Carrascosa PM, Cury RC, García MJ, Leipsic JA (2015-10-03). Dual-Energy CT in Cardiovascular Imaging. Springer. ISBN 978-3-319-21227-2.
- ^ Schmidt B, Flohr T (2020-11-01). "Principles and applications of dual source CT". Physica Medica. 125 Years of X-Rays. 79: 36–46. doi:10.1016/j.ejmp.2020.10.014. ISSN 1120-1797. PMID 33115699. S2CID 226056088.
- ^ a b Seidensticker PR, Hofmann LK (2008-05-24). Dual Source CT Imaging. Springer Science & Business Media. ISBN 978-3-540-77602-4.
- ^ Schmidt B, Flohr T (2020-11-01). "Principles and applications of dual source CT". Physica Medica: European Journal of Medical Physics. 79: 36–46. doi:10.1016/j.ejmp.2020.10.014. ISSN 1120-1797. PMID 33115699. S2CID 226056088.
- ^ Mahmood U, Horvat N, Horvat JV, Ryan D, Gao Y, Carollo G, DeOcampo R, Do RK, Katz S, Gerst S, Schmidtlein CR, Dauer L, Erdi Y, Mannelli L (May 2018). "Rapid Switching kVp Dual Energy CT: Value of Reconstructed Dual Energy CT Images and Organ Dose Assessment in Multiphasic Liver CT Exams". European Journal of Radiology. 102: 102–108. doi:10.1016/j.ejrad.2018.02.022. ISSN 0720-048X. PMC 5918634. PMID 29685522.
- ^ Johnson TR (November 2012). "Dual-Energy CT: General Principles". American Journal of Roentgenology. 199 (5_supplement): S3–S8. doi:10.2214/AJR.12.9116. ISSN 0361-803X. PMID 23097165.
- ^ a b c Wittsack HJ, Wohlschläger A, Ritzl E, Kleiser R, Cohnen M, Seitz R, Mödder U (2008-01-01). "CT-perfusion imaging of the human brain: Advanced deconvolution analysis using circulant singular value decomposition". Computerized Medical Imaging and Graphics. 32 (1): 67–77. doi:10.1016/j.compmedimag.2007.09.004. ISSN 0895-6111. PMID 18029143.
- ^ Williams M, Newby D (2016-08-01). "CT myocardial perfusion imaging: current status and future directions". Clinical Radiology. 71 (8): 739–749. doi:10.1016/j.crad.2016.03.006. ISSN 0009-9260. PMID 27091433.
- ^ a b Donahue J, Wintermark M (2015-02-01). "Perfusion CT and acute stroke imaging: Foundations, applications, and literature review". Journal of Neuroradiology. 42 (1): 21–29. doi:10.1016/j.neurad.2014.11.003. ISSN 0150-9861. PMID 25636991.
- ^ Blodgett TM, Meltzer CC, Townsend DW (February 2007). "PET/CT: form and function". Radiology. 242 (2): 360–385. doi:10.1148/radiol.2422051113. ISSN 0033-8419. PMID 17255408.
- ^ Ciernik I, Dizendorf E, Baumert BG, Reiner B, Burger C, Davis J, Lütolf UM, Steinert HC, Von Schulthess GK (November 2003). "Radiation treatment planning with an integrated positron emission and computer tomography (PET/CT): a feasibility study". International Journal of Radiation Oncology, Biology, Physics. 57 (3): 853–863. doi:10.1016/s0360-3016(03)00346-8. ISSN 0360-3016. PMID 14529793.
- ^ Ul-Hassan F, Cook GJ (August 2012). "PET/CT in oncology". Clinical Medicine. 12 (4): 368–372. doi:10.7861/clinmedicine.12-4-368. ISSN 1470-2118. PMC 4952129. PMID 22930885.
- ^ Curry TS, Dowdey JE, Murry RC (1990). Christensen's Physics of Diagnostic Radiology. Lippincott Williams & Wilkins. p. 289. ISBN 978-0-8121-1310-5.
- ^ "CT Screening" (PDF). hps.org. Archived from the original (PDF) on 13 October 2016. Retrieved 1 May 2018.
- ^ a b Smith-Bindman R, Lipson J, Marcus R, Kim KP, Mahesh M, Gould R, Berrington de González A, Miglioretti DL (December 2009). "Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer". Archives of Internal Medicine. 169 (22): 2078–2086. doi:10.1001/archinternmed.2009.427. PMC 4635397. PMID 20008690.
- ^ a b Berrington de González A, Mahesh M, Kim KP, Bhargavan M, Lewis R, Mettler F, Land C (December 2009). "Projected cancer risks from computed tomographic scans performed in the United States in 2007". Arch. Intern. Med. 169 (22): 2071–7. doi:10.1001/archinternmed.2009.440. PMC 6276814. PMID 20008689.
- ^ "Dangers of CT Scans and X-Rays – Consumer Reports". Retrieved 16 May 2018.
- ^ American Academy of Orthopaedic Surgeons, American College of Emergency Physicians, UMBC (2017-03-20). Critical Care Transport. Jones & Bartlett Learning. p. 389. ISBN 978-1-284-04099-9.
- ^ Galloway R Jr (2015). "Introduction and Historical Perspectives on Image-Guided Surgery". In Golby AJ (ed.). Image-Guided Neurosurgery. Amsterdam: Elsevier. pp. 3–4. ISBN 978-0-12-800870-6.
- ^ Tse V, Kalani M, Adler JR (2015). "Techniques of Stereotactic Localization". In Chin LS, Regine WF (eds.). Principles and Practice of Stereotactic Radiosurgery. New York: Springer. p. 28. ISBN 978-0-387-71070-9.
- ^ Saleh H, Kassas B (2015). "Developing Stereotactic Frames for Cranial Treatment". In Benedict SH, Schlesinger DJ, Goetsch SJ, Kavanagh BD (eds.). Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy. Boca Raton: CRC Press. pp. 156–159. ISBN 978-1-4398-4198-3.
- ^ Khan FR, Henderson JM (2013). "Deep Brain Stimulation Surgical Techniques". In Lozano AM, Hallet M (eds.). Brain Stimulation. Handbook of Clinical Neurology. Vol. 116. Amsterdam: Elsevier. pp. 28–30. doi:10.1016/B978-0-444-53497-2.00003-6. ISBN 978-0-444-53497-2. PMID 24112882.
- ^ Arle J (2009). "Development of a Classic: the Todd-Wells Apparatus, the BRW, and the CRW Stereotactic Frames". In Lozano AM, Gildenberg PL, Tasker RR (eds.). Textbook of Stereotactic and Functional Neurosurgery. Berlin: Springer-Verlag. pp. 456–461. ISBN 978-3-540-69959-0.
- ^ Brown RA, Nelson JA (June 2012). "Invention of the N-localizer for stereotactic neurosurgery and its use in the Brown-Roberts-Wells stereotactic frame". Neurosurgery. 70 (2 Supplement Operative): 173–176. doi:10.1227/NEU.0b013e318246a4f7. PMID 22186842. S2CID 36350612.
- ^ Daniel G Deschler, Joseph Zenga. "Evaluation of a neck mass in adults". UpToDate. This topic last updated: Dec 04, 2017.
- ^ a b Bin Saeedan M, Aljohani IM, Khushaim AO, Bukhari SQ, Elnaas ST (2016). "Thyroid computed tomography imaging: pictorial review of variable pathologies". Insights into Imaging. 7 (4): 601–617. doi:10.1007/s13244-016-0506-5. ISSN 1869-4101. PMC 4956631. PMID 27271508.
- ^ Computed Tomography of the Lung. Springer Berlin Heidelberg. 2007. pp. 40, 47. ISBN 978-3-642-39518-5.
- ^ High-resolution CT of the Lung. Lippincott Williams & Wilkins. 2009. pp. 81, 568. ISBN 978-0-7817-6909-9.
- ^ Martínez-Jiménez S, Rosado-de-Christenson ML, Carter BW (2017-07-22). Specialty Imaging: HRCT of the Lung E-Book. Elsevier Health Sciences. ISBN 978-0-323-52495-7.
- ^ Yuranga Weerakkody. "Bronchial wall thickening". Radiopaedia. Archived from the original on 2018-01-06. Retrieved 2018-01-05.
- ^ Wiener RS, Gould MK, Woloshin S, Schwartz LM, Clark JA (2012). ""What do you mean, a spot?": A qualitative analysis of patients' reactions to discussions with their doctors about pulmonary nodules". Chest. 143 (3): 672–677. doi:10.1378/chest.12-1095. PMC 3590883. PMID 22814873.
- ^ a b c American College of Chest Physicians, American Thoracic Society (September 2013), "Five Things Physicians and Patients Should Question", Choosing Wisely, American College of Chest Physicians and American Thoracic Society, archived from the original on 3 November 2013, retrieved 6 January 2013, which cites
- MacMahon H, Austin JH, Gamsu G, Herold CJ, Jett JR, Naidich DP, Patz EF, Swensen SJ (2005). "Guidelines for Management of Small Pulmonary Nodules Detected on CT Scans: A Statement from the Fleischner Society1". Radiology. 237 (2): 395–400. doi:10.1148/radiol.2372041887. PMID 16244247. S2CID 14498160.
- Gould MK, Fletcher J, Iannettoni MD, Lynch WR, Midthun DE, Naidich DP, Ost DE (2007). "Evaluation of Patients with Pulmonary Nodules: When is It Lung Cancer?*". Chest. 132 (3_suppl): 108S–130S. doi:10.1378/chest.07-1353. PMID 17873164. S2CID 16449420.
- Smith-Bindman R, Lipson J, Marcus R, Kim KP, Mahesh M, Gould R, Berrington de González A, Miglioretti DL (2009). "Radiation Dose Associated with Common Computed Tomography Examinations and the Associated Lifetime Attributable Risk of Cancer". Archives of Internal Medicine. 169 (22): 2078–2086. doi:10.1001/archinternmed.2009.427. PMC 4635397. PMID 20008690.
- Wiener RS, Gould MK, Woloshin S, Schwartz LM, Clark JA (2012). ""What do you mean, a spot?": A qualitative analysis of patients' reactions to discussions with their doctors about pulmonary nodules". Chest. 143 (3): 672–677. doi:10.1378/chest.12-1095. PMC 3590883. PMID 22814873.
- ^ McDermott M, Jacobs T, Morgenstern L (2017-01-01), Wijdicks EF, Kramer AH (eds.), "Chapter 10 – Critical care in acute ischemic stroke", Handbook of Clinical Neurology, Critical Care Neurology Part I, 140, Elsevier: 153–176, doi:10.1016/b978-0-444-63600-3.00010-6, PMID 28187798
- ^ "Computed Tomography Angiography (CTA)". www.hopkinsmedicine.org. 19 November 2019. Retrieved 2021-03-21.
- ^ Zeman RK, Silverman PM, Vieco PT, Costello P (1995-11-01). "CT angiography". American Journal of Roentgenology. 165 (5): 1079–1088. doi:10.2214/ajr.165.5.7572481. ISSN 0361-803X. PMID 7572481.
- ^ Ramalho J, Castillo M (2014-03-31). Vascular Imaging of the Central Nervous System: Physical Principles, Clinical Applications, and Emerging Techniques. John Wiley & Sons. p. 69. ISBN 978-1-118-18875-0.
- ^ Jones DA, Beirne AM, Kelham M, Rathod KS, Andiapen M, Wynne L, Godec T, Forooghi N, Ramaseshan R, Moon JC, Davies C, Bourantas CV, Baumbach A, Manisty C, Wragg A (2023-10-31). "Computed Tomography Cardiac Angiography Before Invasive Coronary Angiography in Patients With Previous Bypass Surgery: The BYPASS-CTCA Trial". Circulation. 148 (18): 1371–1380. doi:10.1161/CIRCULATIONAHA.123.064465. ISSN 0009-7322. PMC 11139242. PMID 37772419.
- ^ "CT scan reduces the complications of angiography after bypass surgery". NIHR Evidence. 6 August 2024. doi:10.3310/nihrevidence_63153.
- ^ "Cardiac CT Scan – NHLBI, NIH". www.nhlbi.nih.gov. Archived from the original on 2017-12-01. Retrieved 2017-11-22.
- ^ a b Wichmann JL. "Cardiac CT | Radiology Reference Article | Radiopaedia.org". radiopaedia.org. Archived from the original on 2017-12-01. Retrieved 2017-11-22.
- ^ Marwan M, Achenbach S (February 2016). "Role of Cardiac CT Before Transcatheter Aortic Valve Implantation (TAVI)". Current Cardiology Reports. 18 (2): 21. doi:10.1007/s11886-015-0696-3. ISSN 1534-3170. PMID 26820560. S2CID 41535442.
- ^ Moss AJ, Dweck MR, Dreisbach JG, Williams MC, Mak SM, Cartlidge T, Nicol ED, Morgan-Hughes GJ (2016-11-01). "Complementary role of cardiac CT in the assessment of aortic valve replacement dysfunction". Open Heart. 3 (2): e000494. doi:10.1136/openhrt-2016-000494. ISSN 2053-3624. PMC 5093391. PMID 27843568.
- ^ Thériault-Lauzier P, Spaziano M, Vaquerizo B, Buithieu J, Martucci G, Piazza N (September 2015). "Computed Tomography for Structural Heart Disease and Interventions". Interventional Cardiology Review. 10 (3): 149–154. doi:10.15420/ICR.2015.10.03.149. ISSN 1756-1477. PMC 5808729. PMID 29588693.
- ^ Passariello R (2006-03-30). Multidetector-Row CT Angiography. Springer Science & Business Media. ISBN 978-3-540-26984-7.
- ^ Radiological Society of North America, American College of Radiology. "Coronary Computed Tomography Angiography (CCTA)". www.radiologyinfo.org. Retrieved 2021-03-19.
- ^ "Heart scan (coronary calcium scan)". Mayo Clinic. Archived from the original on 5 September 2015. Retrieved 9 August 2015.
- ^ van der Bijl N, Joemai RM, Geleijns J, Bax JJ, Schuijf JD, de Roos A, Kroft LJ (2010). "Assessment of Agatston Coronary Artery Calcium Score Using Contrast-Enhanced CT Coronary Angiography". American Journal of Roentgenology. 195 (6): 1299–1305. doi:10.2214/AJR.09.3734. ISSN 0361-803X. PMID 21098187.
- ^ Vukicevic M, Mosadegh B, Min JK, Little SH (February 2017). "Cardiac 3D Printing and its Future Directions". JACC: Cardiovascular Imaging. 10 (2): 171–184. doi:10.1016/j.jcmg.2016.12.001. ISSN 1876-7591. PMC 5664227. PMID 28183437.
- ^ Wang DD, Eng M, Greenbaum A, Myers E, Forbes M, Pantelic M, Song T, Nelson C, Divine G, Taylor A, Wyman J, Guerrero M, Lederman RJ, Paone G, O'Neill W (2016). "Innovative Mitral Valve Treatment with 3D Visualization at Henry Ford". JACC: Cardiovascular Imaging. 9 (11): 1349–1352. doi:10.1016/j.jcmg.2016.01.017. PMC 5106323. PMID 27209112. Archived from the original on 2017-12-01. Retrieved 2017-11-22.
- ^ Wang DD, Eng M, Greenbaum A, Myers E, Forbes M, Pantelic M, Song T, Nelson C, Divine G (November 2016). "Predicting LVOT Obstruction After TMVR". JACC: Cardiovascular Imaging. 9 (11): 1349–1352. doi:10.1016/j.jcmg.2016.01.017. ISSN 1876-7591. PMC 5106323. PMID 27209112.
- ^ Jacobs S, Grunert R, Mohr FW, Falk V (February 2008). "3D-Imaging of cardiac structures using 3D heart models for planning in heart surgery: a preliminary study". Interactive Cardiovascular and Thoracic Surgery. 7 (1): 6–9. doi:10.1510/icvts.2007.156588. ISSN 1569-9285. PMID 17925319.
- ^ Furukawa A, Saotome T, Yamasaki M, Maeda K, Nitta N, Takahashi M, Tsujikawa T, Fujiyama Y, Murata K, Sakamoto T (2004-05-01). "Cross-sectional Imaging in Crohn Disease". RadioGraphics. 24 (3): 689–702. doi:10.1148/rg.243035120. ISSN 0271-5333. PMID 15143222.
- ^ CT of the Acute Abdomen. Springer Berlin Heidelberg. 2011. p. 37. ISBN 978-3-540-89232-8.
- ^ Jay P Heiken, Douglas S Katz (2014). "Emergency Radiology of the Abdomen and Pelvis: Imaging of the Nontraumatic and Traumatic Acute Abdomen". In J. Hodler, R. A. Kubik-Huch, G. K. von Schulthess, Ch. L. Zollikofer (eds.). Diseases of the Abdomen and Pelvis. Springer Milan. p. 3. ISBN 978-88-470-5659-6.
- ^ Skolarikos A, Neisius A, Petřík A, Somani B, Thomas K, Gambaro G (March 2022). EAU Guidelines on Urolithiasis. Amsterdam: European Association of Urology. ISBN 978-94-92671-16-5.
- ^ Miller OF, Kane CJ (September 1999). "Time to stone passage for observed ureteral calculi: a guide for patient education". Journal of Urology. 162 (3 Part 1): 688–691. doi:10.1097/00005392-199909010-00014. PMID 10458343.
- ^ "Ankle Fractures". orthoinfo.aaos.org. American Association of Orthopedic Surgeons. Archived from the original on 30 May 2010. Retrieved 30 May 2010.
- ^ Buckwalter, Kenneth A., et al. (11 September 2000). "Musculoskeletal Imaging with Multislice CT". American Journal of Roentgenology. 176 (4): 979–986. doi:10.2214/ajr.176.4.1760979. PMID 11264094.
- ^ Ramon A, Bohm-Sigrand A, Pottecher P, Richette P, Maillefert JF, Devilliers H, Ornetti P (2018-03-01). "Role of dual-energy CT in the diagnosis and follow-up of gout: systematic analysis of the literature". Clinical Rheumatology. 37 (3): 587–595. doi:10.1007/s10067-017-3976-z. ISSN 0770-3198. PMID 29350330. S2CID 3686099.
- ^ Keaveny TM (March 2010). "Biomechanical computed tomography-noninvasive bone strength analysis using clinical computed tomography scans". Annals of the New York Academy of Sciences. 1192 (1): 57–65. Bibcode:2010NYASA1192...57K. doi:10.1111/j.1749-6632.2009.05348.x. ISSN 1749-6632. PMID 20392218. S2CID 24132358.
- ^ Barber A, Tozzi G, Pani M (2019-03-07). Computed Tomography Based Biomechanics. Frontiers Media SA. p. 20. ISBN 978-2-88945-780-9.
- ^ Evans LM, Margetts L, Casalegno V, Lever LM, Bushell J, Lowe T, Wallwork A, Young P, Lindemann A (2015-05-28). "Transient thermal finite element analysis of CFC–Cu ITER monoblock using X-ray tomography data". Fusion Engineering and Design. 100: 100–111. Bibcode:2015FusED.100..100E. doi:10.1016/j.fusengdes.2015.04.048. hdl:10871/17772. Archived from the original on 2015-10-16.
- ^ Payne, Emma Marie (2012). "Imaging Techniques in Conservation" (PDF). Journal of Conservation and Museum Studies. 10 (2): 17–29. doi:10.5334/jcms.1021201.
- ^ P. Babaheidarian, D. Castanon (2018). "Joint reconstruction and material classification in spectral CT". In Greenberg JA, Gehm ME, Neifeld MA, Ashok A (eds.). Anomaly Detection and Imaging with X-Rays (ADIX) III. p. 12. doi:10.1117/12.2309663. ISBN 978-1-5106-1775-9. S2CID 65469251.
- ^ P. Jin, E. Haneda, K. D. Sauer, C. A. Bouman (June 2012). "A model-based 3D multi-slice helical CT reconstruction algorithm for transportation security application" (PDF). Second International Conference on Image Formation in X-Ray Computed Tomography. Archived from the original (PDF) on 2015-04-11. Retrieved 2015-04-05.
- ^ P. Jin, E. Haneda, C. A. Bouman (November 2012). "Implicit Gibbs prior models for tomographic reconstruction" (PDF). Signals, Systems and Computers (ASILOMAR), 2012 Conference Record of the Forty Sixth Asilomar Conference on. IEEE. pp. 613–636. Archived from the original (PDF) on 2015-04-11. Retrieved 2015-04-05.
- ^ S. J. Kisner, P. Jin, C. A. Bouman, K. D. Sauer, W. Garms, T. Gable, S. Oh, M. Merzbacher, S. Skatter (October 2013). "Innovative data weighting for iterative reconstruction in a helical CT security baggage scanner" (PDF). Security Technology (ICCST), 2013 47th International Carnahan Conference on. IEEE. Archived from the original (PDF) on 2015-04-10. Retrieved 2015-04-05.
- ^ Megherbi, N., Flitton, G.T., Breckon, T.P. (September 2010). "A Classifier based Approach for the Detection of Potential Threats in CT based Baggage Screening" (PDF). Proc. International Conference on Image Processing. IEEE. pp. 1833–1836. CiteSeerX 10.1.1.188.5206. doi:10.1109/ICIP.2010.5653676. ISBN 978-1-4244-7992-4. S2CID 3679917. Retrieved 5 November 2013.[permanent dead link]
- ^ Megherbi, N., Han, J., Flitton, G.T., Breckon, T.P. (September 2012). "A Comparison of Classification Approaches for Threat Detection in CT based Baggage Screening" (PDF). Proc. International Conference on Image Processing. IEEE. pp. 3109–3112. CiteSeerX 10.1.1.391.2695. doi:10.1109/ICIP.2012.6467558. ISBN 978-1-4673-2533-2. S2CID 6924816. Retrieved 5 November 2013.[permanent dead link]
- ^ Flitton, G.T., Breckon, T.P., Megherbi, N. (September 2013). "A Comparison of 3D Interest Point Descriptors with Application to Airport Baggage Object Detection in Complex CT Imagery" (PDF). Pattern Recognition. 46 (9): 2420–2436. Bibcode:2013PatRe..46.2420F. doi:10.1016/j.patcog.2013.02.008. hdl:1826/15213. S2CID 3687379. Retrieved 5 November 2013.[permanent dead link]
- ^ "Laboratory | About Chikyu | The Deep-sea Scientific Drilling Vessel CHIKYU". www.jamstec.go.jp. Retrieved 2019-10-24.
- ^ Tonai S, Kubo Y, Tsang MY, Bowden S, Ide K, Hirose T, Kamiya N, Yamamoto Y, Yang K, Yamada Y, Morono Y (2019). "A New Method for Quality Control of Geological Cores by X-Ray Computed Tomography: Application in IODP Expedition 370". Frontiers in Earth Science. 7. doi:10.3389/feart.2019.00117. hdl:2164/12811. ISSN 2296-6463. S2CID 171394807.
- ^ Cunningham JA, Rahman IA, Lautenschlager S, Rayfield EJ, Donoghue PC (2014). "A virtual world of paleontology". Trends in Ecology & Evolution. 29 (6): 347–357. doi:10.1016/j.tree.2014.04.004. hdl:20.500.11850/96966. ISSN 0169-5347.
- ^ Seales WB, Parker CS, Segal M, Tov E, Shor P, Porath Y (2016). "From damage to discovery via virtual unwrapping: Reading the scroll from En-Gedi". Science Advances. 2 (9): e1601247. Bibcode:2016SciA....2E1247S. doi:10.1126/sciadv.1601247. ISSN 2375-2548. PMC 5031465. PMID 27679821.
- ^ Castellanos S (2 March 2021). "A Letter Sealed for Centuries Has Been Read—Without Even Opening It". The Wall Street Journal. Retrieved 2 March 2021.
- ^ Dambrogio J, Ghassaei A, Staraza Smith D, Jackson H, Demaine ML (2 March 2021). "Unlocking history through automated virtual unfolding of sealed documents imaged by X-ray microtomography". Nature Communications. 12 (1): 1184. Bibcode:2021NatCo..12.1184D. doi:10.1038/s41467-021-21326-w. PMC 7925573. PMID 33654094.
- ^ Advanced documentation methods in studying Corinthian black-figure vase painting on YouTube showing a Computed Tomography scan and rollout of the aryballos No. G26, archaeological collection, Graz University. The video was rendered using the GigaMesh Software Framework, cf. doi:10.11588/heidok.00025189. Karl S, Bayer P, Mara H, Márton A (2019), "Advanced Documentation Methods in Studying Corinthian Black-figure Vase Painting" (PDF), Proceedings of the 23rd International Conference on Cultural Heritage and New Technologies (CHNT23), Vienna, Austria, ISBN 978-3-200-06576-5, retrieved 2020-01-09
- ^ "CT FOR ART". NICAS. Retrieved 2023-07-04.
- ^ Bulcke JV, Boone M, Acker JV, Hoorebeke LV (October 2009). "Three-Dimensional X-Ray Imaging and Analysis of Fungi on and in Wood". Microscopy and Microanalysis. 15 (5): 395–402. Bibcode:2009MiMic..15..395V. doi:10.1017/S1431927609990419. hdl:1854/LU-675607. ISSN 1435-8115. PMID 19709462. S2CID 15637414.
- ^ Goldman LW (2008). "Principles of CT: Multislice CT". Journal of Nuclear Medicine Technology. 36 (2): 57–68. doi:10.2967/jnmt.107.044826. ISSN 0091-4916. PMID 18483143.
- ^ a b Reis EP, Nascimento F, Aranha M, Mainetti Secol F, Machado B, Felix M, Stein A, Amaro E (29 July 2020). "Brain Hemorrhage Extended (BHX): Bounding box extrapolation from thick to thin slice CT images v1.1". PhysioNet. 101 (23): 215–220. doi:10.13026/9cft-hg92.
- ^ Park S, Chu L, Hruban R, Vogelstein B, Kinzler K, Yuille A, Fouladi D, Shayesteh S, Ghandili S, Wolfgang C, Burkhart R, He J, Fishman E, Kawamoto S (2020-09-01). "Differentiating autoimmune pancreatitis from pancreatic ductal adenocarcinoma with CT radiomics features". Diagnostic and Interventional Imaging. 101 (9): 555–564. doi:10.1016/j.diii.2020.03.002. ISSN 2211-5684. PMID 32278586. S2CID 215751181.
- ^ a b Fishman EK, Ney DR, Heath DG, Corl FM, Horton KM, Johnson PT (2006). "Volume Rendering versus Maximum Intensity Projection in CT Angiography: What Works Best, When, and Why". RadioGraphics. 26 (3): 905–922. doi:10.1148/rg.263055186. ISSN 0271-5333. PMID 16702462.
- ^ Silverstein JC, Parsad NM, Tsirline V (2008). "Automatic perceptual color map generation for realistic volume visualization". Journal of Biomedical Informatics. 41 (6): 927–935. doi:10.1016/j.jbi.2008.02.008. ISSN 1532-0464. PMC 2651027. PMID 18430609.
- ^ Kobbelt L (2006). Vision, Modeling, and Visualization 2006: Proceedings, November 22-24, 2006, Aachen, Germany. IOS Press. p. 185. ISBN 978-3-89838-081-2.
- ^ a b Computerized Tomography chapter Archived 2016-03-04 at the Wayback Machine at University of Connecticut Health Center.
- ^ Schmidt D, Odland R (September 2004). "Mirror-Image Reversal of Coronal Computed Tomography Scans". The Laryngoscope. 114 (9): 1562–1565. doi:10.1097/00005537-200409000-00011. ISSN 0023-852X. PMID 15475782. S2CID 22320649.
- ^ Brant and Helms' fundamentals of diagnostic radiology (Fifth ed.). Lippincott Williams & Wilkins. 2018-07-19. p. 1600. ISBN 978-1-4963-6738-9. Retrieved 24 January 2019.
- ^ Arthur W. Toga, John C. Mazziotta, eds. (2002). Brain mapping: the methods (2nd ed.). Amsterdam: Academic Press. ISBN 0-12-693019-8. OCLC 52594824.
- ^ Jerrold T. Bushberg, J. Anthony Seibert, Edwin M. Leidholdt, John M. Boone (2002). The essential physics of medical imaging (2nd ed.). Philadelphia, PA: Lippincott Williams & Wilkins. p. 358. ISBN 0-683-30118-7. OCLC 47177732.
- ^ Kamalian S, Lev MH, Gupta R (2016-01-01). "Computed tomography imaging and angiography – principles". Neuroimaging Part I. Handbook of Clinical Neurology. Vol. 135. pp. 3–20. doi:10.1016/B978-0-444-53485-9.00001-5. ISBN 978-0-444-53485-9. ISSN 0072-9752. PMID 27432657.
- ^ Stirrup J (2020-01-02). Cardiovascular Computed Tomography. Oxford University Press. p. 136. ISBN 978-0-19-880927-2.
- ^ Carroll QB (2007). Practical Radiographic Imaging. Charles C Thomas Publisher. p. 512. ISBN 978-0-398-08511-7.
- ^ Udupa JK, Herman GT (1999-09-28). 3D Imaging in Medicine, Second Edition. CRC Press. ISBN 978-0-8493-3179-4.
- ^ Krupski W, Kurys-Denis E, Matuszewski Ł, Plezia B (2007-06-30). "Use of multi-planar reconstruction (MPR) and 3-dimentional [sic] (3D) CT to assess stability criteria in C2 vertebral fractures". Journal of Pre-Clinical and Clinical Research. 1 (1): 80–83. ISSN 1898-2395.
- ^ Tins B (2010-10-21). "Technical aspects of CT imaging of the spine". Insights into Imaging. 1 (5–6): 349–359. doi:10.1007/s13244-010-0047-2. ISSN 1869-4101. PMC 3259341. PMID 22347928.
- ^ "CT imaging: Where are we going? (Proceedings)". DVM 360. April 2010. Retrieved 2021-03-21.
- ^ Wolfson N, Lerner A, Roshal L (2016-05-30). Orthopedics in Disasters: Orthopedic Injuries in Natural Disasters and Mass Casualty Events. Springer. ISBN 978-3-662-48950-5.
- ^ Laroia AT, Thompson BH, Laroia ST, van Beek EJ (2010-07-28). "Modern imaging of the tracheo-bronchial tree". World Journal of Radiology. 2 (7): 237–248. doi:10.4329/wjr.v2.i7.237. ISSN 1949-8470. PMC 2998855. PMID 21160663.
- ^ Gong JS, Xu JM (2004-07-01). "Role of curved planar reformations using multidetector spiral CT in diagnosis of pancreatic and peripancreatic diseases". World Journal of Gastroenterology. 10 (13): 1943–1947. doi:10.3748/wjg.v10.i13.1943. ISSN 1007-9327. PMC 4572236. PMID 15222042.
- ^ Dalrymple NC, Prasad SR, Freckleton MW, Chintapalli KN (September 2005). "Informatics in radiology (infoRAD): introduction to the language of three-dimensional imaging with multidetector CT". Radiographics. 25 (5): 1409–1428. doi:10.1148/rg.255055044. ISSN 1527-1323. PMID 16160120.
- ^ Calhoun PS, Kuszyk BS, Heath DG, Carley JC, Fishman EK (1999-05-01). "Three-dimensional Volume Rendering of Spiral CT Data: Theory and Method". RadioGraphics. 19 (3): 745–764. doi:10.1148/radiographics.19.3.g99ma14745. ISSN 0271-5333. PMID 10336201.
- ^ van Ooijen PM, van Geuns RJ, Rensing BJ, Bongaerts AH, de Feyter PJ, Oudkerk M (January 2003). "Noninvasive Coronary Imaging Using Electron Beam CT: Surface Rendering Versus Volume Rendering". American Journal of Roentgenology. 180 (1): 223–226. doi:10.2214/ajr.180.1.1800223. ISSN 0361-803X. PMID 12490509.
- ^ R. A. Crowther, D. J. DeRosier, A. Klug (1970). "The Reconstruction of a Three-Dimensional Structure from Projections and its Application to Electron Microscopy". Proc. R. Soc. Lond. A. 317 (1530): 319–340. Bibcode:1970RSPSA.317..319C. doi:10.1098/rspa.1970.0119. S2CID 122980366.
- ^ Nickoloff EL, Alderson PO (August 2001). "Radiation Exposures to Patients from CT: Reality, Public Perception, and Policy". American Journal of Roentgenology. 177 (2): 285–287. doi:10.2214/ajr.177.2.1770285. ISSN 0361-803X. PMID 11461846.
- ^ Barkan, O; Weill, J; Averbuch, A; Dekel, S. "Adaptive Compressed Tomography Sensing" Archived 2016-03-13 at the Wayback Machine. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition 2013 (pp. 2195–2202).
- ^ Proceedings. IEEE. 1995. p. 10. ISBN 978-0-7803-2498-5.
- ^ "Radiation – Effects on organs of the body (somatic effects)". Encyclopedia Britannica. Retrieved 2021-03-21.
- ^ Simpson G (2009). "Thoracic computed tomography: principles and practice". Australian Prescriber. 32 (4): 4. doi:10.18773/austprescr.2009.049.
- ^ a b Hsieh J (2003). Computed Tomography: Principles, Design, Artifacts, and Recent Advances. SPIE Press. p. 167. ISBN 978-0-8194-4425-7.
- ^ Bhowmik UK, Zafar Iqbal, M., Adhami, Reza R. (28 May 2012). "Mitigating motion artifacts in FDK based 3D Cone-beam Brain Imaging System using markers". Central European Journal of Engineering. 2 (3): 369–382. Bibcode:2012CEJE....2..369B. doi:10.2478/s13531-012-0011-7.
- ^ a b P. Jin, C. A. Bouman, K. D. Sauer (2013). "A Method for Simultaneous Image Reconstruction and Beam Hardening Correction" (PDF). IEEE Nuclear Science Symp. & Medical Imaging Conf., Seoul, Korea, 2013. Archived from the original (PDF) on 2014-06-06. Retrieved 2014-04-23.
- ^ Boas FE, Fleischmann D (2011). "Evaluation of Two Iterative Techniques for Reducing Metal Artifacts in Computed Tomography". Radiology. 259 (3): 894–902. doi:10.1148/radiol.11101782. PMID 21357521.
- ^ Mouton, A., Megherbi, N., Van Slambrouck, K., Nuyts, J., Breckon, T.P. (2013). "An Experimental Survey of Metal Artefact Reduction in Computed Tomography" (PDF). Journal of X-Ray Science and Technology. 21 (2): 193–226. doi:10.3233/XST-130372. hdl:1826/8204. PMID 23694911.[permanent dead link]
- ^ Pessis E, Campagna R, Sverzut JM, Bach F, Rodallec M, Guerini H, Feydy A, Drapé JL (2013). "Virtual Monochromatic Spectral Imaging with Fast Kilovoltage Switching: Reduction of Metal Artifacts at CT". RadioGraphics. 33 (2): 573–583. doi:10.1148/rg.332125124. ISSN 0271-5333. PMID 23479714.
- ^ González Ballester MA, Zisserman AP, Brady M (December 2002). "Estimation of the partial volume effect in MRI". Medical Image Analysis. 6 (4): 389–405. doi:10.1016/s1361-8415(02)00061-0. ISSN 1361-8415. PMID 12494949.
- ^ Goldszal AF, Pham DL (2000-01-01). "Volumetric Segmentation". Handbook of Medical Imaging: 185–194. doi:10.1016/B978-012077790-7/50016-3. ISBN 978-0-12-077790-7.
- ^ a b Jha D (2014). "Adaptive center determination for effective suppression of ring artifacts in tomography images". Applied Physics Letters. 105 (14): 143107. Bibcode:2014ApPhL.105n3107J. doi:10.1063/1.4897441.
- ^ Van Nieuwenhove V, De Beenhouwer J, De Carlo F, Mancini L, Marone F, Sijbers J (2015). "Dynamic intensity normalization using eigen flat fields in X-ray imaging" (PDF). Optics Express. 23 (21): 27975–27989. Bibcode:2015OExpr..2327975V. doi:10.1364/oe.23.027975. hdl:10067/1302930151162165141. PMID 26480456.
- ^ Sijbers J, Postnov A (2004). "Reduction of ring artefacts in high resolution micro-CT reconstructions". Phys Med Biol. 49 (14): N247–53. doi:10.1088/0031-9155/49/14/N06. PMID 15357205. S2CID 12744174.
- ^ Newton TH, Potts DG (1971). Radiology of the Skull and Brain: Technical aspects of computed tomography. Mosby. pp. 3941–3950. ISBN 978-0-8016-3662-2.
- ^ Brüning R, Küttner A, Flohr T (2006-01-16). Protocols for Multislice CT. Springer Science & Business Media. ISBN 978-3-540-27273-1.
- ^ Peh WC (2017-08-11). Pitfalls in Musculoskeletal Radiology. Springer. ISBN 978-3-319-53496-1.
- ^ Van de Casteele E, Van Dyck D, Sijbers J, Raman E (2004). "A model-based correction method for beam hardening artefacts in X-ray microtomography". Journal of X-ray Science and Technology. 12 (1): 43–57. CiteSeerX 10.1.1.460.6487.
- ^ Van Gompel G, Van Slambrouck K, Defrise M, Batenburg KJ, Sijbers J, Nuyts J (2011). "Iterative correction of beam hardening artifacts in CT". Medical Physics. 38 (1): 36–49. Bibcode:2011MedPh..38S..36V. CiteSeerX 10.1.1.464.3547. doi:10.1118/1.3577758. PMID 21978116.
- ^ Mikla VI, Mikla VV (2013-08-23). Medical Imaging Technology. Elsevier. p. 37. ISBN 978-0-12-417036-0.
- ^ Radiology for the Dental Professional. Elsevier Mosby. 2008. p. 337. ISBN 978-0-323-03071-7.
- ^ Pasipoularides A (November 2009). Heart's Vortex: Intracardiac Blood Flow Phenomena. PMPH-USA. p. 595. ISBN 978-1-60795-033-2.
- ^ Heiken JP, Peterson CM, Menias CO (November 2005). "Virtual colonoscopy for colorectal cancer screening: current status: Wednesday 5 October 2005, 14:00–16:00". Cancer Imaging. 5 (Spec No A). International Cancer Imaging Society: S133–S139. doi:10.1102/1470-7330.2005.0108. PMC 1665314. PMID 16361129.
- ^ Bielen DJ, Bosmans HT, De Wever LL, Maes F, Tejpar S, Vanbeckevoort D, Marchal GJ (September 2005). "Clinical validation of high-resolution fast spin-echo MR colonography after colon distention with air". J Magn Reson Imaging. 22 (3): 400–5. doi:10.1002/jmri.20397. PMID 16106357. S2CID 22167728.
- ^ "CT Colonography". Radiologyinfo.org.
- ^ Žabić S, Wang Q, Morton T, Brown KM (March 2013). "A low dose simulation tool for CT systems with energy integrating detectors". Medical Physics. 40 (3): 031102. Bibcode:2013MedPh..40c1102Z. doi:10.1118/1.4789628. PMID 23464282.
- ^ Brian R. Subach M.D., F.A.C.S et al."Reliability and accuracy of fine-cut computed tomography scans to determine the status of anterior interbody fusions with metallic cages" Archived 2012-12-08 at the Wayback Machine
- ^ a b c d e f g Brenner DJ, Hall EJ (November 2007). "Computed tomography – an increasing source of radiation exposure" (PDF). N. Engl. J. Med. 357 (22): 2277–84. doi:10.1056/NEJMra072149. PMID 18046031. S2CID 2760372. Archived (PDF) from the original on 2016-03-04.
- ^ a b c Redberg, Rita F., and Smith-Bindman, Rebecca. "We Are Giving Ourselves Cancer" Archived 2017-07-06 at the Wayback Machine, New York Times, January 30, 2014
- ^ Health Cf. "Medical X-ray Imaging – What are the Radiation Risks from CT?". www.fda.gov. Archived from the original on 5 November 2013. Retrieved 1 May 2018.
- ^ Radiological Society of North America, American College of Radiology (February 2021). "Patient Safety – Radiation Dose in X-Ray and CT Exams" (PDF). acr.org. Archived from the original (PDF) on 1 January 2021. Retrieved 6 April 2021.
- ^ Mathews JD, Forsythe AV, Brady Z, Butler MW, Goergen SK, Byrnes GB, Giles GG, Wallace AB, Anderson PR, Guiver TA, McGale P, Cain TM, Dowty JG, Bickerstaffe AC, Darby SC (2013). "Cancer risk in 680 000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians". BMJ. 346 (may21 1): f2360. doi:10.1136/bmj.f2360. ISSN 1756-1833. PMC 3660619. PMID 23694687.
- ^ Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, Howe NL, Ronckers CM, Rajaraman P, Sir Craft AW, Parker L, Berrington de González A (4 August 2012). "Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study". Lancet. 380 (9840): 499–505. doi:10.1016/S0140-6736(12)60815-0. PMC 3418594. PMID 22681860.
- ^ Meulepas JM, Ronckers CM, Smets AM, Nievelstein RA, Gradowska P, Lee C, Jahnen A, van Straten M, de Wit MC, Zonnenberg B, Klein WM, Merks JH, Visser O, van Leeuwen FE, Hauptmann M (1 March 2019). "Radiation Exposure From Pediatric CT Scans and Subsequent Cancer Risk in the Netherlands". JNCI: Journal of the National Cancer Institute. 111 (3): 256–263. doi:10.1093/jnci/djy104. PMC 6657440. PMID 30020493.
- ^ de Gonzalez AB, Salotti JA, McHugh K, Little MP, Harbron RW, Lee C, Ntowe E, Braganza MZ, Parker L, Rajaraman P, Stiller C, Stewart DR, Craft AW, Pearce MS (February 2016). "Relationship between paediatric CT scans and subsequent risk of leukaemia and brain tumours: assessment of the impact of underlying conditions". British Journal of Cancer. 114 (4): 388–394. doi:10.1038/bjc.2015.415. PMC 4815765. PMID 26882064.
- ^ Smoll NR, Brady Z, Scurrah KJ, Lee C, Berrington de González A, Mathews JD (14 January 2023). "Computed tomography scan radiation and brain cancer incidence". Neuro-Oncology. 25 (7): 1368–1376. doi:10.1093/neuonc/noad012. PMC 10326490. PMID 36638155.
- ^ Sasieni PD, Shelton J, Ormiston-Smith N, Thomson CS, Silcocks PB (2011). "What is the lifetime risk of developing cancer?: the effect of adjusting for multiple primaries". British Journal of Cancer. 105 (3): 460–465. doi:10.1038/bjc.2011.250. ISSN 0007-0920. PMC 3172907. PMID 21772332.
- ^ a b c Rehani MM, Yang K, Melick ER, Heil J, Šalát D, Sensakovic WF, Liu B (2020). "Patients undergoing recurrent CT scans: assessing the magnitude". European Radiology. 30 (4): 1828–1836. doi:10.1007/s00330-019-06523-y. PMID 31792585. S2CID 208520824.
- ^ a b Brambilla M, Vassileva J, Kuchcinska A, Rehani MM (2020). "Multinational data on cumulative radiation exposure of patients from recurrent radiological procedures: call for action". European Radiology. 30 (5): 2493–2501. doi:10.1007/s00330-019-06528-7. PMID 31792583. S2CID 208520544.
- ^ a b Rehani MM, Melick ER, Alvi RM, Doda Khera R, Batool-Anwar S, Neilan TG, Bettmann M (2020). "Patients undergoing recurrent CT exams: assessment of patients with non-malignant diseases, reasons for imaging and imaging appropriateness". European Radiology. 30 (4): 1839–1846. doi:10.1007/s00330-019-06551-8. PMID 31792584. S2CID 208520463.
- ^ Eckel LJ, Fletcher JG, Bushberg JT, McCollough CH (2015-10-01). "Answers to Common Questions About the Use and Safety of CT Scans". Mayo Clinic Proceedings. 90 (10): 1380–1392. doi:10.1016/j.mayocp.2015.07.011. ISSN 0025-6196. PMID 26434964.
- ^ "Expert opinion: Are CT scans safe?". ScienceDaily. Retrieved 2019-03-14.
- ^ McCollough CH, Bushberg JT, Fletcher JG, Eckel LJ (2015-10-01). "Answers to Common Questions About the Use and Safety of CT Scans". Mayo Clinic Proceedings. 90 (10): 1380–1392. doi:10.1016/j.mayocp.2015.07.011. ISSN 0025-6196. PMID 26434964.
- ^ "No evidence that CT scans, X-rays cause cancer". Medical News Today. 4 February 2016. Retrieved 2019-03-14.
- ^ Kalra MK, Maher MM, Rizzo S, Kanarek D, Shephard JA (April 2004). "Radiation exposure from Chest CT: Issues and Strategies". Journal of Korean Medical Science. 19 (2): 159–166. doi:10.3346/jkms.2004.19.2.159. ISSN 1011-8934. PMC 2822293. PMID 15082885.
- ^ Rob S, Bryant T, Wilson I, Somani B (2017). "Ultra-low-dose, low-dose, and standard-dose CT of the kidney, ureters, and bladder: is there a difference? Results from a systematic review of the literature". Clinical Radiology. 72 (1): 11–15. doi:10.1016/j.crad.2016.10.005. PMID 27810168.
- ^ a b c d e f g h i j k l m n o p Whaites E (2008-10-10). Radiography and Radiology for Dental Care Professionals E-Book. Elsevier Health Sciences. p. 25. ISBN 978-0-7020-4799-2.
- ^ a b c d e Davies HE, Wathen, C. G., Gleeson, F. V. (25 February 2011). "The risks of radiation exposure related to diagnostic imaging and how to minimise them". BMJ. 342 (feb25 1): d947. doi:10.1136/bmj.d947. PMID 21355025. S2CID 206894472.
- ^ Baysson H, Etard C, Brisse HJ, Bernier MO (January 2012). "[Diagnostic radiation exposure in children and cancer risk: current knowledge and perspectives]". Archives de Pédiatrie. 19 (1): 64–73. doi:10.1016/j.arcped.2011.10.023. PMID 22130615.
- ^ a b c d Semelka RC, Armao DM, Elias J, Huda W (May 2007). "Imaging strategies to reduce the risk of radiation in CT studies, including selective substitution with MRI". J Magn Reson Imaging. 25 (5): 900–9. doi:10.1002/jmri.20895. PMID 17457809. S2CID 5788891.
- ^ Larson DB, Rader SB, Forman HP, Fenton LZ (August 2007). "Informing parents about CT radiation exposure in children: it's OK to tell them". Am J Roentgenol. 189 (2): 271–5. doi:10.2214/AJR.07.2248. PMID 17646450. S2CID 25020619.
- ^ Emmerson B, Young M (2023), "Radiology Patient Safety and Communication", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 33620790, retrieved 2023-11-24
- ^ a b Namasivayam S, Kalra MK, Torres WE, Small WC (Jul 2006). "Adverse reactions to intravenous iodinated contrast media: a primer for radiologists". Emergency Radiology. 12 (5): 210–5. doi:10.1007/s10140-006-0488-6. PMID 16688432. S2CID 28223134.
- ^ a b c Christiansen C (2005-04-15). "X-ray contrast media – an overview". Toxicology. 209 (2): 185–7. Bibcode:2005Toxgy.209..185C. doi:10.1016/j.tox.2004.12.020. PMID 15767033.
- ^ a b Wang H, Wang HS, Liu ZP (October 2011). "Agents that induce pseudo-allergic reaction". Drug Discov Ther. 5 (5): 211–9. doi:10.5582/ddt.2011.v5.5.211. PMID 22466368. S2CID 19001357.
- ^ Drain KL, Volcheck GW (2001). "Preventing and managing drug-induced anaphylaxis". Drug Safety. 24 (11): 843–53. doi:10.2165/00002018-200124110-00005. PMID 11665871. S2CID 24840296.
- ^ Castells MC, ed. (2010-12-09). Anaphylaxis and hypersensitivity reactions. New York: Humana Press. p. 187. ISBN 978-1-60327-950-5.
- ^ a b c Hasebroock KM, Serkova NJ (April 2009). "Toxicity of MRI and CT contrast agents". Expert Opinion on Drug Metabolism & Toxicology. 5 (4): 403–16. doi:10.1517/17425250902873796. PMID 19368492. S2CID 72557671.
- ^ Rawson JV, Pelletier AL (2013-09-01). "When to Order Contrast-Enhanced CT". American Family Physician. 88 (5): 312–316. ISSN 0002-838X. PMID 24010394.
- ^ Thomsen HS, Muller RN, Mattrey RF (2012-12-06). Trends in Contrast Media. Springer Science & Business Media. ISBN 978-3-642-59814-2.
- ^ Davenport M (2020). "Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation". Radiology. 294 (3): 660–668. doi:10.1148/radiol.2019192094. PMID 31961246.
- ^ a b c Cuttler JM, Pollycove M (2009). "Nuclear energy and health: and the benefits of low-dose radiation hormesis". Dose-Response. 7 (1): 52–89. doi:10.2203/dose-response.08-024.Cuttler. PMC 2664640. PMID 19343116.
- ^ a b "What are the Radiation Risks from CT?". Food and Drug Administration. 2009. Archived from the original on 2013-11-05.
- ^ a b c d e f Hall EJ, Brenner DJ (May 2008). "Cancer risks from diagnostic radiology". The British Journal of Radiology. 81 (965): 362–78. doi:10.1259/bjr/01948454. PMID 18440940. S2CID 23348032.
- ^ a b c d e Shrimpton, P.C; Miller, H.C; Lewis, M.A; Dunn, M. Doses from Computed Tomography (CT) examinations in the UK – 2003 Review Archived 2011-09-22 at the Wayback Machine
- ^ Michael T. Ryan, Poston, John W., eds. (2005). A half century of health physics. Baltimore, Md.: Lippincott Williams & Wilkins. p. 164. ISBN 978-0-7817-6934-1.
- ^ Polo SE, Jackson SP (March 2011). "Dynamics of DNA damage response proteins at DNA breaks: a focus on protein modifications". Genes Dev. 25 (5): 409–33. doi:10.1101/gad.2021311. PMC 3049283. PMID 21363960.
- ^ The Measurement, Reporting, and Management of Radiation Dose in CT Archived 2017-06-23 at the Wayback Machine "It is a single dose parameter that reflects the risk of a nonuniform exposure in terms of an equivalent whole-body exposure."
- ^ Hill B, Venning AJ, Baldock C (2005). "A preliminary study of the novel application of normoxic polymer gel dosimeters for the measurement of CTDI on diagnostic X-ray CT scanners". Medical Physics. 32 (6): 1589–1597. Bibcode:2005MedPh..32.1589H. doi:10.1118/1.1925181. PMID 16013718.
- ^ Issa ZF, Miller JM, Zipes DP (2019-01-01). "Complications of Catheter Ablation of Cardiac Arrhythmias". Clinical Arrhythmology and Electrophysiology. Elsevier. pp. 1042–1067. doi:10.1016/b978-0-323-52356-1.00032-3. ISBN 978-0-323-52356-1.
- ^ "Absorbed, Equivalent, and Effective Dose – ICRPaedia". icrpaedia.org. Retrieved 2021-03-21.
- ^ Materials NR (1999). Radiation Quantities and Units, Definitions, Acronyms. National Academies Press (US).
- ^ Pua BB, Covey AM, Madoff DC (2018-12-03). Interventional Radiology: Fundamentals of Clinical Practice. Oxford University Press. ISBN 978-0-19-027624-9.
- ^ Paragraph 55 in: "The 2007 Recommendations of the International Commission on Radiological Protection". International Commission on Radiological Protection. Archived from the original on 2012-11-16. Ann. ICRP 37 (2-4)
- ^ "Do CT scans cause cancer?". Harvard Medical School. March 2013. Archived from the original on 2017-12-09. Retrieved 2017-12-09.
- ^ CDC (2020-06-05). "Radiation and pregnancy: A fact sheet for clinicians". Centers for Disease Control and Prevention. Retrieved 2021-03-21.
- ^ Yoon I, Slesinger TL (2021), "Radiation Exposure In Pregnancy", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 31869154, retrieved 2021-03-21
- ^ Wintermark M, Lev MH (January 2010). "FDA investigates the safety of brain perfusion CT". AJNR Am J Neuroradiol. 31 (1): 2–3. doi:10.3174/ajnr.A1967. PMC 7964089. PMID 19892810.
- ^ a b Whitley SA, Dodgeon J, Meadows A, Cullingworth J, Holmes K, Jackson M, Hoadley G, Kulshrestha R (2020-01-06). Clark's Procedures in Diagnostic Imaging: A System-Based Approach. CRC Press. ISBN 978-1-4987-1552-2.
- ^ Tippins R, Torres WE, Baumgartner B, Baumgarten D (August 2000). "Are screening serum creatinine levels necessary prior to outpatient CT examinations?". Radiology. 216 (2): 481–484. doi:10.1148/radiology.216.2.r00au23481. ISSN 0033-8419. PMID 10924574.
- ^ Jun K, Yoon S (2017). "Alignment Solution for CT Image Reconstruction using Fixed Point and Virtual Rotation Axis". Scientific Reports. 7: 41218. arXiv:1605.04833. Bibcode:2017NatSR...741218J. doi:10.1038/srep41218. ISSN 2045-2322. PMC 5264594. PMID 28120881.
- ^ "Computed Tomography (CT)". www.nibib.nih.gov. Retrieved 2021-03-20.
- ^ Aichinger H, Dierker J, Joite-Barfuß S, Säbel M (2011-10-25). Radiation Exposure and Image Quality in X-Ray Diagnostic Radiology: Physical Principles and Clinical Applications. Springer Science & Business Media. p. 5. ISBN 978-3-642-11241-6.
- ^ Erdoğan H (1999). Statistical Image Reconstruction Algorithms Using Paraboloidal Surrogates for PET Transmission Scans. University of Michigan. ISBN 978-0-599-63374-2.
- ^ Themes UF (2018-10-07). "CT Image Reconstruction Basics". Radiology Key. Retrieved 2021-03-20.
- ^ a b Stirrup J (2020-01-02). Cardiovascular Computed Tomography. Oxford University Press. ISBN 978-0-19-880927-2.
- ^ "computed tomography – Definition from the Merriam-Webster Online Dictionary". Archived from the original on 19 September 2011. Retrieved 18 August 2009.
- ^ Webb WR, Brant WE, Major NM (2014). Fundamentals of Body CT. Elsevier Health Sciences. p. 152. ISBN 978-0-323-26358-0.
- ^ Webb WR, Brant WE, Major NM (2006-01-01). Fundamentals of Body CT. Elsevier Health Sciences. p. 168. ISBN 978-1-4160-0030-3.
- ^ Thomas AM, Banerjee AK, Busch U (2005-12-05). Classic Papers in Modern Diagnostic Radiology. Springer Science & Business Media. ISBN 978-3-540-26988-5.
- ^ Radon J (1 December 1986). "On the determination of functions from their integral values along certain manifolds". IEEE Transactions on Medical Imaging. 5 (4): 170–176. doi:10.1109/TMI.1986.4307775. PMID 18244009. S2CID 26553287.
- ^ Oldendorf WH (1978). "The quest for an image of brain: a brief historical and technical review of brain imaging techniques". Neurology. 28 (6): 517–33. doi:10.1212/wnl.28.6.517. PMID 306588. S2CID 42007208.
- ^ Richmond C (2004). "Obituary – Sir Godfrey Hounsfield". BMJ. 329 (7467): 687. doi:10.1136/bmj.329.7467.687. PMC 517662.
- ^ Pietzsch J. "The Nobel Prize in Physiology or Medicine 1979". NobelPrize.org.
- ^ Frank Natterer (2001). The Mathematics of Computerized Tomography (Classics in Applied Mathematics). Society for Industrial and Applied Mathematics. p. 8. ISBN 978-0-89871-493-7.
- ^ Sperry L (2015-12-14). Mental Health and Mental Disorders: An Encyclopedia of Conditions, Treatments, and Well-Being [3 volumes]: An Encyclopedia of Conditions, Treatments, and Well-Being. ABC-CLIO. p. 259. ISBN 978-1-4408-0383-3.
- ^ Hounsfield GN (1977). "The E.M.I. Scanner". Proceedings of the Royal Society of London. Series B, Biological Sciences. 195 (1119): 281–289. Bibcode:1977RSPSB.195..281H. doi:10.1098/rspb.1977.0008. ISSN 0080-4649. JSTOR 77187. PMID 13396. S2CID 34734270.
- ^ Miñano G (3 November 2015). "What's the difference between a CAT-Scan and a CT-Scan? - Cincinnati Children's Blog". blog.cincinnatichildrens.org. Archived from the original on 2022-06-17. Retrieved 2021-03-19.
- ^ "Difference Between CT Scan and CAT Scan | Difference Between". 28 January 2010. Retrieved 2021-03-19.
- ^ Conquer Your Headaches. International Headache Management. 1994. p. 115. ISBN 978-0-9636292-5-8.
- ^ "MeSH Browser". meshb.nlm.nih.gov.
- ^ Edholm P, Gabor H (December 1987). "Linograms in Image Reconstruction from Projections". IEEE Transactions on Medical Imaging. MI-6 (4): 301–7. doi:10.1109/tmi.1987.4307847. PMID 18244038. S2CID 20832295.
- ^ "Computed tomography (CT) scanners". OECD.
- ^ "Image Gently". The Alliance for Radiation Safety in Pediatric Imaging. Archived from the original on 9 June 2013. Retrieved 19 July 2013.
- ^ "Image Wisely". Joint Task Force on Adult Radiation Protection. Archived from the original on 21 July 2013. Retrieved 19 July 2013.
- ^ "Optimal levels of radiation for patients". World Health Organization. Archived from the original on 25 May 2013. Retrieved 19 July 2013.
- ^ "Global Initiative on Radiation Safety in Healthcare Settings" (PDF). World Health Organization. Archived (PDF) from the original on 29 October 2013. Retrieved 19 July 2013.
- ^ Fred A. Mettler Jr, Mythreyi Bhargavan, Keith Faulkner, Debbie B. Gilley, Joel E. Gray, Geoffrey S. Ibbott, Jill A. Lipoti, Mahadevappa Mahesh, John L. McCrohan, Michael G. Stabin, Bruce R. Thomadsen, Terry T. Yoshizumi (2009). "Radiologic and Nuclear Medicine Studies in the United States and Worldwide: Frequency, Radiation Dose, and Comparison with Other Radiation Sources — 1950-2007". Radiology. 253 (2): 520–531. doi:10.1148/radiol.2532082010. PMID 19789227.
- ^ Andrew Skelly (Aug 3, 2010). "CT ordering all over the map". The Medical Post.
- ^ Korley FK, Pham JC, Kirsch TD (October 2010). "Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998–2007". JAMA. 304 (13): 1465–71. doi:10.1001/jama.2010.1408. PMID 20924012.
- ^ "Global Computed Tomography (CT) Scanners Devices and Equipment Market Report 2020: Major Players are GE Healthcare, Koninklijke Philips, Hitachi, Siemens and Canon Medical Systems – ResearchAndMarkets.com". Business Wire. November 7, 2019.
- ^ Jenkins R, Gould RW, Gedcke D (1995). "Instrumentation". Quantitative x-ray spectrometry (2nd ed.). New York: Dekker. p. 90. ISBN 978-0-8247-9554-2.
- ^ Shikhaliev PM, Xu T, Molloi S (2005). "Photon counting computed tomography: Concept and initial results". Medical Physics. 32 (2): 427–36. Bibcode:2005MedPh..32..427S. doi:10.1118/1.1854779. PMID 15789589.
- ^ Taguchi K, Iwanczyk JS (2013). "Vision 20/20: Single photon counting x-ray detectors in medical imaging". Medical Physics. 40 (10): 100901. Bibcode:2013MedPh..40j0901T. doi:10.1118/1.4820371. PMC 3786515. PMID 24089889.
- ^ "NIH uses photon-counting CT scanner in patients for the first time". National Institutes of Health. 24 February 2016. Archived from the original on 18 August 2016. Retrieved 28 July 2016.
- ^ "Photon-counting breast CT measures up". medicalphysicsweb. Archived from the original on 2016-07-27. Retrieved 28 July 2016.
- ^ Kachelrieß M, Rehani MM (March 1, 2020). "Is it possible to kill the radiation risk issue in computed tomography?". Physica Medica: European Journal of Medical Physics. 71: 176–177. doi:10.1016/j.ejmp.2020.02.017. PMID 32163886. S2CID 212692606 – via www.physicamedica.com.
External links
[edit]- Development of CT imaging
- CT Artefacts—PPT by David Platten
- Filler A (2009-06-30). "The History, Development and Impact of Computed Imaging in Neurological Diagnosis and Neurosurgery: CT, MRI, and DTI". Nature Precedings: 1. doi:10.1038/npre.2009.3267.4. ISSN 1756-0357.
- Boone JM, McCollough CH (2021). "Computed tomography turns 50". Physics Today. 74 (9): 34–40. Bibcode:2021PhT....74i..34B. doi:10.1063/PT.3.4834. ISSN 0031-9228. S2CID 239718717.